IOM 2009 Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 5 Were Legally Registered and the Ones That Had Identified, 194 Were Not in the Register Were Found Operational by the Census Team
A SACCO Annual General Meeting in Lango, Northern Uganda Chapter Five SACCOs and MFIs 125 5.1 Failing SACCOs: Who Cares?1 Visiting a member of MAMIDECOT, a successfully managed SACCO in Masaka. Section 1 Evidence of Failure Why should anybody care about failing, – thus SACCOs seldom live their “full missing or untraceable SACCOs? Are not lives”. They therefore do not serve their institutions, like biological organisms, full purpose before dying. supposed to be subject to the immutable ii) In the remote rural areas, SACCOs are law of entropy? Are they not supposed to be often the only providers of financial born, grow, decline and die? And, given this services for most people. When the pattern, should the failing of SACCOs be an SACCOs fail, this leaves people with issue? little or no alternative services. There are three principal reasons why we iii) SACCO collapses leave people poorer should all be concerned about the failure rate and more desperate as they lose their of SACCOs in Uganda: meager savings i) Whereas in countries like Kenya the iv) Losing their money in failing SACCOs life of a SACCO spans over decades, makes poor people more cynical of the failure rate in Uganda suggests that using financial institutions. Such a most SACCOs fail after only a few years 1 Author: Andrew Obara, FRIENDS Consult 126 polluting effect entrenches financial iii. While the census team was remarkably exclusion as more low-income / poor thorough, there may have been some people get discouraged from accessing institutions which exist but were simply financial institutions’ services. -

DISTRICT BASELINE: Nakasongola, Nakaseke and Nebbi in Uganda
EASE – CA PROJECT PARTNERS EAST AFRICAN CIVIL SOCIETY FOR SUSTAINABLE ENERGY & CLIMATE ACTION (EASE – CA) PROJECT DISTRICT BASELINE: Nakasongola, Nakaseke and Nebbi in Uganda SEPTEMBER 2019 Prepared by: Joint Energy and Environment Projects (JEEP) P. O. Box 4264 Kampala, (Uganda). Supported by Tel: +256 414 578316 / 0772468662 Email: [email protected] JEEP EASE CA PROJECT 1 Website: www.jeepfolkecenter.org East African Civil Society for Sustainable Energy and Climate Action (EASE-CA) Project ALEF Table of Contents ACRONYMS ......................................................................................................................................... 4 ACKNOWLEDGEMENT .................................................................................................................... 5 EXECUTIVE SUMMARY .................................................................................................................. 6 CHAPTER ONE: INTRODUCTION ................................................................................................. 8 1.1 Background of JEEP ............................................................................................................ 8 1.2 Energy situation in Uganda .................................................................................................. 8 1.3 Objectives of the baseline study ......................................................................................... 11 1.4 Report Structure ................................................................................................................ -

18 Magado Ronald Article
GEROLD RAHMANN, VICTOR OLOWE, TIMOTHY OLABIYI, KHALID AZIM, OLUGBENGA ADEOLUWA (Eds.) (2018) Scientific Track Proceedings of the 4TH African Organic Conference. “Ecological and Organic Agriculture Strategies for Viable Continental and National Development in the Context of the African Union's Agenda 2063”. November 5-8, 2018. Saly Portudal, Senegal Impact of Climate Change on Cassava Farming a Case study of Wabinyonyi Sub county Nakasongola District Magado Ronald and Abstract Ssekyewa Charles Cassava is a potential crop to improve the livelihood of people but findings from Nakasongola District this research through conducting interviews from respondents show that 97.8% Farmers Association, responded that climate change contributed to the decline in yield. There is increased P.O Box 1, Nakasongola incidences of pest and diseases that cause rotting of the tubers that are the economic District, Uganda part used by the people. The study recommends that the Government of Uganda should strengthen climate change issues through line ministries such as Ministry of Agriculture, Animal Industries and Fisheries, Ministry of Lands, Housing and Corresponding author: Urban development; Ministry of Water and Environment in terms of policies to [email protected] support the development of smallholder farmers during this era of climate change. Nakasongola District Local Government and its development partners should strengthen agricultural service delivery in all areas particularly climate Keywords: change smart agriculture and much attention should be put on cassava value Climate change, chain from production, value addition and marketing as a high value crop for mitigation mechanism, both food security and income generation. mixed cropping system, cassava, food security Introduction Cassava is widely grown and has the potential to alleviate poverty in Uganda. -

Ending CHILD MARRIAGE and TEENAGE PREGNANCY in Uganda
ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA Final Report - December 2015 ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA 1 A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA Final Report - December 2015 ACKNOWLEDGEMENTS The United Nations Children Fund (UNICEF) gratefully acknowledges the valuable contribution of many individuals whose time, expertise and ideas made this research a success. Gratitude is extended to the Research Team Lead by Dr. Florence Kyoheirwe Muhanguzi with support from Prof. Grace Bantebya Kyomuhendo and all the Research Assistants for the 10 districts for their valuable support to the research process. Lastly, UNICEF would like to acknowledge the invaluable input of all the study respondents; women, men, girls and boys and the Key Informants at national and sub national level who provided insightful information without whom the study would not have been accomplished. I ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA CONTENTS ACKNOWLEDGEMENTS ..................................................................................I -

Mapping a Healthier Future
Health Planning Department, Ministry of Health, Uganda Directorate of Water Development, Ministry of Water and Environment, Uganda Uganda Bureau of Statistics International Livestock Research Institute World Resources Institute The Republic of Uganda Health Planning Department MINISTRY OF HEALTH, UGANDA Directorate of Water Development MINISTRY OF WATER AND ENVIRONMENT, UGANDA Uganda Bureau of Statistics Mapping a Healthier Future ISBN: 978-1-56973-728-6 How Spatial Analysis Can Guide Pro-Poor Water and Sanitation Planning in Uganda HEALTH PLANNING DEPARTMENT MINISTRY OF HEALTH, UGANDA Plot 6 Lourdel Road P.O. Box 7272 AUTHORS AND CONTRIBUTORS Kampala, Uganda http://www.health.go.ug/ This publication was prepared by a core team from fi ve institutions: The Health Planning Department at the Ministry of Health (MoH) leads eff orts to provide strategic support Health Planning Department, Ministry of Health, Uganda to the Health Sector in achieving sector goals and objectives. Specifi cally, the Planning Department guides Paul Luyima sector planning; appraises and monitors programmes and projects; formulates, appraises and monitors Edward Mukooyo national policies and plans; and appraises regional and international policies and plans to advise the sector Didacus Namanya Bambaiha accordingly. Francis Runumi Mwesigye Directorate of Water Development, Ministry of Water and Environment, Uganda DIRECTORATE OF WATER DEVELOPMENT Richard Cong MINISTRY OF WATER AND ENVIRONMENT, UGANDA Plot 21/28 Port Bell Road, Luzira Clara Rudholm P.O. Box 20026 Disan Ssozi Kampala, Uganda Wycliff e Tumwebaze http://www.mwe.go.ug/MoWE/13/Overview Uganda Bureau of Statistics The Directorate of Water Development (DWD) is the lead government agency for the water and sanitation Thomas Emwanu sector under the Ministry of Water and Environment (MWE) with the mandate to promote and ensure the rational and sustainable utilization, development and safeguard of water resources for social and economic Bernard Justus Muhwezi development, as well as for regional and international peace. -
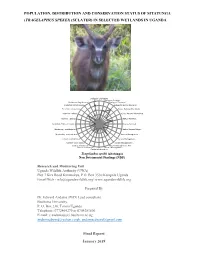
Population, Distribution and Conservation Status of Sitatunga (Tragelaphus Spekei) (Sclater) in Selected Wetlands in Uganda
POPULATION, DISTRIBUTION AND CONSERVATION STATUS OF SITATUNGA (TRAGELAPHUS SPEKEI) (SCLATER) IN SELECTED WETLANDS IN UGANDA Biological -Life history Biological -Ecologicl… Protection -Regulation of… 5 Biological -Dispersal Protection -Effectiveness… 4 Biological -Human tolerance Protection -proportion… 3 Status -National Distribtuion Incentive - habitat… 2 Status -National Abundance Incentive - species… 1 Status -National… Incentive - Effect of harvest 0 Status -National… Monitoring - confidence in… Status -National Major… Monitoring - methods used… Harvest Management -… Control -Confidence in… Harvest Management -… Control - Open access… Harvest Management -… Control of Harvest-in… Harvest Management -Aim… Control of Harvest-in… Harvest Management -… Control of Harvest-in… Tragelaphus spekii (sitatunga) NonSubmitted Detrimental to Findings (NDF) Research and Monitoring Unit Uganda Wildlife Authority (UWA) Plot 7 Kira Road Kamwokya, P.O. Box 3530 Kampala Uganda Email/Web - [email protected]/ www.ugandawildlife.org Prepared By Dr. Edward Andama (PhD) Lead consultant Busitema University, P. O. Box 236, Tororo Uganda Telephone: 0772464279 or 0704281806 E-mail: [email protected] [email protected], [email protected] Final Report i January 2019 Contents ACRONYMS, ABBREVIATIONS, AND GLOSSARY .......................................................... vii EXECUTIVE SUMMARY ....................................................................................................... viii 1.1Background ........................................................................................................................... -

A Prolonged Cholera Outbreak Caused by Drinking Contaminated Stream Water, Kyangwali Refugee Settlement, Hoima District, Western Uganda: 2018
A prolonged cholera outbreak caused by drinking contaminated stream water, Kyangwali Refugee Settlement, Hoima District, Western Uganda: 2018 Fred Monje ( [email protected] ) Uganda Public Health Fellowship Program https://orcid.org/0000-0002-8786-2695 Alex Riolexus Ario Uganda Public Health Fellowship Program Angella Musewa Uganda Public Health Fellowship Program Kenneth Bainomugisha Uganda Public Health Fellowship Program Bernadette Basuta Mirembe Uganda Public Health Fellowship Program Dativa Maria Aliddeki Uganda Public Health Fellowship Program Daniel Eurien Uganda Public Health Fellowship Program Godfrey Nsereko Uganda Public Health Fellowship Program Carol Nanziri Uganda Public Health Fellowship Program Esther Kisaakye Uganda Public Health Fellowship Program Vivian Ntono Uganda Public Health Fellowship Program Benon Kwesiga Uganda Public Health Fellowship Program Daniel Kadobera Uganda Public Health Fellowship Program Lilian Bulage Uganda Public Health Fellowship Program Godfrey Bwire Ministry of Health Patrick Tusiime Page 1/21 Ministry of Health Julie Harris Uganda Public Health Fellowship Program Bao-Ping Zhu Chronic Diseases Research Article Keywords: Outbreak, Cholera, Refugees, Uganda Posted Date: September 14th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-36121/v3 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on November 4th, 2020. See the published version at https://doi.org/10.1186/s40249-020-00761-9. Page 2/21 Abstract Background: On 23 February 2018, the Uganda Ministry of Health (MOH) declared a cholera outbreak affecting more than 60 persons in Kyangwali Refugee Settlement, Hoima District, bordering the Democratic Republic of Congo (DRC). -

Country Operations Plan
COUNTRY OPERATIONS PLAN Country: Uganda Planning Year: 2004 2004 Country Operations Plan – Uganda __________________________________________________________________________________________ Part I: Executive - Summary 1.1 Context and Beneficiary Populations UNHCR’s presence in Uganda dates back from the 1960s. Though the earlier arrivals of Rwandan refugees had returned in 1994, the country still hosts 18,500 Rwandans who are residual caseloads of the 1996 repatriation from Tanzania. There are some 5,000 Rwandans who entered Mbarara district of Uganda from Tanzania when the Rwandan refugees were being repatriated from there in 2002. The Government of Uganda has not yet decided their status. The majority of the refugees in the country today are Southern Sudanese hosted in northern Uganda and who number about 172,300 (86%) of the total refugee population of 200,800 as of 28 February 2003. About 8,500 Congolese refugees hosted in the Southwest are from the Democratic Republic of Congo (DRC). There are other smaller groups from Somalia, Ethiopia and Kenya that are also being assisted. Sudanese and Congolese refugees are granted status on a prima facie basis, while the status of others is ascertained through individual refugee status determination. Almost all the refugees fled their respective countries of origin because of the civil war and fear of persecution caused by ethnic rivalries and political differences. The Government of Uganda, continues to host refugees from the neighbouring countries. Refugees who are in designated settlememnts are provided with agricultural lands, tools and seeds with the objective of making them self-sufficient. As a result, refugees in the northern settlements have managed to produce a certain percentage of their food requirements, thereby reducing dependence on the food assistance from WFP. -

Kasese District Profile.Indd
THE REPUBLIC OF UGANDA Kasese District Hazard, Risk and Vulnerability Profi le 2016 Kasese District Hazard, Risk and Vulnerability Profi le a b Kasese District Hazard, Risk and Vulnerability Profile Contents List of Tables.........................................................................................................................ii List of Figures......................................................................................................................... ii Acknowledgment .................................................................................................................. iii Executive Summary ............................................................................................................. iv Acronyms ............................................................................................................................ vi Definition of Terms .............................................................................................................. vii Introduction .......................................................................................................................... 1 Objectives ............................................................................................................................ 1 Methodology ........................................................................................................................ 1 District Overview ................................................................................................................. -

Generosity in the Time of Covid Vol 4
VOLUME 4 A Compilation of stories on Giving in the time of the Covid-19 Pandemic in Uganda Period Covered August-September 2020 About CivSource Africa CivSource Africa is a philanthropy support and advisory organization committed to nurturing a more sustainable, effective and connected civil society that advances the dignity and voices of all people. We do this through promoting reflective, responsive, and accountable philanthropic practice. CivSource Africa is also passionate about promoting African philanthropy and telling the stories of African giving and generosity. Plot 18, Balikuddembe Road, Naguru Kampala, Uganda P.O Box 4310 Tel: +256 393 224 056 civsourceafrica.com [email protected] https://www.facebook.com/CivSourceAfrica https://twitter.com/CivsourceAfrica Table of Contents 5 Foreword 6 Acknowledgements 7 Acronyms 8 Background Chapter 1 9 Corporate Giving Chapter 2 15 Giving In Crisis Chapter 3 19 Public To The Rescue Chapter 6 Chapter 4 32 Children: A Tale Of 22 Donating Much-Needed Blood Adorable Givers Chapter 7 38 Giving Within The Arts Chapter 8 42 Giving Information Chapter 9 45 Thinking Post-Coronavirus Chapter 5 24 Giving To Special Groups Chapter 10 47 Outside The Ugandan Borders Foreword e are honored to bring you consistently showcase how all kinds Wthe forth and final installment of individuals and communities are of the “Generosity During COVID” expressing generosity, especially reports. during the COVID-19 pandemic. It has been a true pleasure looking We think it is important to shift for and recounting these stories and that gaze in a way that enables us to expressions of Ugandan generosity, acknowledge and also think about community solidarity and Ubuntu. -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

Strengthening National Feedback and Grievance Redress Mechanism for Uganda’S Redd+ Programme
STRENGTHENING NATIONAL FEEDBACK AND GRIEVANCE REDRESS MECHANISM FOR UGANDA’S REDD+ PROGRAMME (Contract No. MWE/SRVCS/14-15/00018) DRAFT REPORT TO BE SUBMITTED TO THE MINISTRY OF WATER AND ENVIRONMENT CONSULTANT: ADVOCATES COALITION FOR DEVELOPMENT AND ENVIRONMENT (ACODE) PLOT 96, KANJOKYA STREET, KAMWOKYA. P. O. BOX 29836, KAMPALA - UGANDA. TEL: +256312812150, http://www.acode-u.org/ Email: [email protected] , [email protected] Submission Date: 27 September 2016 1 ACKNOWLEDGEMENT Uganda’s REDD+ study for the development of the National Feedback and Grievance Redress Mechanism (FGRM) was undertaken by the Advocates’ Coalition for Development and the Environment (ACODE) on the behalf of the Ministry of Water and Environment (MoW&E). The study process was funded by the World Bank. The study was commissioned and overseen by the REDD+ Secretariat under the Forest Sector Support Department (FSSD) on behalf of the Ministry. The MW&E is grateful to all the efforts of all these key partners in the entire process. During the preparation of the proposed FGRM, MW&E immensely benefited from the invaluable contribution of the Strategic Environmental and Social Assessment (SESA) Taskforce convened by the FSSD and the REDD+ Secretariat, among other ongoing REDD+ assessments. In addition, MW&E benefited from the input of ACODE’s FGRM taskforce comprising an array of experts drawn from areas relevant to the study scope. The Taskforce not only made a significant contribution to the development of the draft inception report but also reviewed and made invaluable comments to the draft report. MW&E would like to thank the team of researchers who mobilised the communities and fully participated in the data collection processes.