Fisd/Uil Certificate for Athletics Instructions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
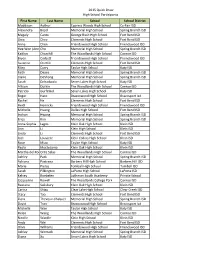
2015 Quick Draw High School Participants First Name Last Name
2015 Quick Draw High School Participants First Name Last Name School School District Maddison Authur Cypress Woods High School Cy-Fair ISD Alexandra Boyd Memorial High School Spring Branch ISD Magaly Cantu George Bush High School Fort Bend ISD Gina Chee Clements High School Fort Bend ISD Anna Chen Friendswood High School Friendswood ISD Hee Won (AnnaCho Memorial High School Spring Branch ISD Kaitlyn Churchill The Woodlands High School Conroe ISD Bryce Corbett Friendswood High School Friendswood ISD Suzanne Ctvrtlik Clements High School Fort Bend ISD Riley Curry Taylor High School Katy ISD Faith Deans Memorial High School Spring Branch ISD Claire DeShong Memorial High School Spring Branch ISD Sarah Dohadwala Seven Lakes High School Katy ISD Allison Durkin The Woodlands High School Conroe ISD Patricia Gurfinkel Seven Lakes High School Katy ISD Roger Haro Brazoswood High School Brazosport Isd Rachel He Clements High School Fort Bend ISD Heidi Henricks Friendswood High School Friendswood ISD Michelle Huang Dulles High School Fort Bend ISD Inchan Hwang Memorial High School Spring Branch ISD Erica Kim Memorial High School Spring Branch ISD Anna-Sophia Lagos Klein Oak High School Klein ISD Ann Li Klein High School Klein ISD Linda Li Clements High School Fort Bend ISD Joel Louviere Klein Collins High School Klein ISD Rose Miao Taylor High School Katy ISD Paola Moctezuma Klein Oak High School Klein ISD Martha del RocOrtiz Salas The Woodlands High School Conroe ISD Ashley Park Memorial High School Spring Branch ISD Adriana Pastrana Barbers Hill -

AVCA High School All-Region
AVCA High School All-Region Region First Name Last Name Height Position High School Name City State College Commitment 1 Emily Dempsey 6'0 OH Avon High School Avon CT 1 Sadie Budzik 5’6 OH Cromwell High School Cromwell CT 1 Cierra Yim 5'2 S Dartmouth High School Dartmouth MA 1 Angie Grabmeier 5'6 S/RS Hopkinton High School Hopkinton MA 1 Melissa Morelli 5'10 S/RS Lynnfield High School Lynnfield MA 1 Aleeya Jones 5'9 OH Wiscasset Christian Academy Wiscasset ME 1 Emma Wheeler 5'9 MB Inter-Lakes High School Meredith NH Connecticut College 1 Tamara Pichardo 5'9 S/RS Clarkstown South High School West Nyack NY 1 Sadie Sharkey 5'6 DS/L Corning Painted Post High School Corning NY University of North Carolina at Wilmington 1 Rosanna Bradica 6'0 MB Francis Lewis High School Fresh Meadow NY 1 Avery Snyder 5'4 DS/L Horseheads High School Horseheads NY Coastal Carolina Lacrosse 1 Maggie Cafrey 5'6 S Kellenberg Memorial High School Uniondale NY 1 Gabriella Heimbauer OH Massapequa High School West Hempstead NY 1 Cecilia Dignan 5'6 S Millbrook High School Millbrook NY SUNY Geneseo 1 Brianna Culcay 5'5 S/RS Ossining High School Ossining NY 1 Mychael Vernon 5'11 OH Ossining High School Ossining NY Oregon State 1 Samantha Cox 5'8 OH Pierson/bridgehampton Sag Harbor NY 1 Taylor Pannell 6'0 MB Pine Bush High School Pine Bush NY University of Connecticut 1 Magan Chin 5'10 OH Scarsdale High School Scarsdale NY 1 Isabelle Smith 5'8 DS/L Westhampton Beach High School Westhampton Beach NY 2 Nicole Taylor 5'11 OH St. -
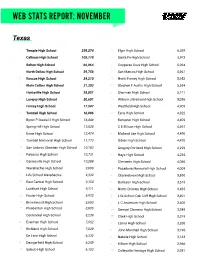
Web Stats Report: November
WEB STATS REPORT: NOVEMBER Texas 1 Temple High School 259,274 31 Elgin High School 6,029 2 Calhoun High School 108,778 32 Santa Fe High School 5,973 3 Belton High School 66,064 33 Copperas Cove High School 5,964 4 North Dallas High School 59,756 34 San Marcos High School 5,961 5 Roscoe High School 34,210 35 North Forney High School 5,952 6 Klein Collins High School 31,303 36 Stephen F Austin High School 5,554 7 Huntsville High School 28,851 37 Sherman High School 5,211 8 Lovejoy High School 20,601 38 William J Brennan High School 5,036 9 Forney High School 17,597 39 Westfield High School 4,909 10 Tomball High School 16,986 40 Early High School 4,822 11 Byron P Steele I I High School 16,448 41 Kempner High School 4,809 12 Spring Hill High School 13,028 42 C E Ellison High School 4,697 13 Ennis High School 12,474 43 Midland Lee High School 4,490 14 Tomball Memorial High School 11,773 44 Odem High School 4,470 15 San Antonio Christian High School 10,783 45 Gregory-Portland High School 4,299 16 Palacios High School 10,731 46 Hays High School 4,235 17 Gainesville High School 10,288 47 Clements High School 4,066 18 Waxahachie High School 9,609 48 Pasadena Memorial High School 4,009 19 Life School Waxahachie 9,332 49 Channelview High School 3,890 20 East Central High School 9,150 50 Burleson High School 3,615 21 Lockhart High School 9,111 51 North Crowley High School 3,485 22 Foster High School 8,972 52 Life School Oak Cliff High School 3,401 23 Brownwood High School 8,803 53 L C Anderson High School 3,400 24 Pleasanton High School 8,605 54 Samuel -

Houston Area (Week I) Districts 4 & 6
Houston Area (Week I) Districts 4 & 6 Monday, October 3, 2005 Morning 8:30 AM-11:30 AM Bellville High School Allene Schmitt Austin County Fairgrounds Tele: 979-865-7081 Hwy 159 East - Fairgrounds Pavillion [email protected] Bellville, TX 77418 Includes: Brazos & Sealy HS 8:30 AM-10:30 AM New Caney High School Ann Kramer 21650 Loop 494 Tele: 281-354-3505 New Caney, TX 77357 [email protected] 9:00 AM-10:30 AM New Waverly High School Kaye Nichols 355 Front St. Tele: 936-344-2251 New Waverly, TX 77358 [email protected] Afternoon 1:00 PM-2:30 PM Shepherd High School Julie Willis 1401 S. Byrd Tele: 936-628-3371 Shepherd, TX 77371 [email protected] Includes: Big Sandy, Goodrich and Tarkington HS 12:30 PM-2:30 PM Splendora High School Maidlen Smoot 23747 FM 2090 Tele: 281-689-8008 Splendora, TX 77372 [email protected] Evening 5:00 PM-7:30 PM Brenham High School Fran Gore 525 A H Ehrig Dr. Tele: 979-277-6570 X1141 Brenham, TX 77833 [email protected] 6:00 PM-8:00 PM Huntsville High School Diane Ratliff 441 FM 2821 East Tele: 936-294-7649 Huntsville, TX 77320 [email protected] Includes: Madisonville, Normangee, North Zulch and Trinity HS 6:00 PM-7:30 PM Livingston High School Sandra Gilbert #1 Lions Ave. Tele: 936-328-2250 Livingston, TX 77351 [email protected] Includes: Big Sandy, Corrigan, Goodrich, Leggett and Onalaska HS 7:00 PM-9:00 PM Waller High School Alice Stewart 20950 Field Store Road Tele: 936-931-4032 Waller, TX 77484 [email protected] Tuesday, October 4, 2005 Morning 9:00 AM-10:30 AM Cleveland High School Sandy Williamson 2000 E. -
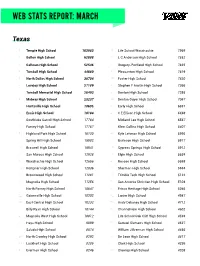
Web Stats Report: March
WEB STATS REPORT: MARCH Texas 1 Temple High School 163983 31 Life School Waxahachie 7969 2 Belton High School 62888 32 L C Anderson High School 7852 3 Calhoun High School 52546 33 Gregory-Portland High School 7835 4 Tomball High School 44880 34 Pleasanton High School 7619 5 North Dallas High School 38704 35 Foster High School 7420 6 Lovejoy High School 27189 36 Stephen F Austin High School 7366 7 Tomball Memorial High School 26493 37 Denton High School 7295 8 Midway High School 23237 38 Denton Guyer High School 7067 9 Huntsville High School 18605 39 Early High School 6881 10 Ennis High School 18184 40 C E Ellison High School 6698 11 Southlake Carroll High School 17784 41 Midland Lee High School 6567 12 Forney High School 17767 42 Klein Collins High School 6407 13 Highland Park High School 16130 43 Kyle Lehman High School 5995 14 Spring Hill High School 15982 44 Burleson High School 5917 15 Braswell High School 15941 45 Cypress Springs High School 5912 16 San Marcos High School 12928 46 Elgin High School 5634 17 Waxahachie High School 12656 47 Roscoe High School 5598 18 Kempner High School 12036 48 Sherman High School 5564 19 Brownwood High School 11281 49 Trimble Tech High School 5122 20 Magnolia High School 11256 50 San Antonio Christian High School 5104 21 North Forney High School 10647 51 Frisco Heritage High School 5046 22 Gainesville High School 10302 52 Lanier High School 4987 23 East Central High School 10232 53 Andy Dekaney High School 4712 24 Billy Ryan High School 10144 54 Channelview High School 4602 25 Magnolia West High School -

Southern Association of Colleges and Schools Commission on Colleges Accreditation Actions Taken by the SACSCOC Board of Trustees September 3, 2020
Southern Association of Colleges and Schools Commission on Colleges Accreditation Actions taken by the SACSCOC Board of Trustees September 3, 2020 At its meeting on September 3, 2020, the SACSCOC Board of Trustees took the following actions regarding the accreditation status of institutions: The Board reaffirmed the accreditation of the following institutions: Atlanta Technical College, Atlanta, GA Belmont Abbey College, Belmont, NC Bevill State Community College, Jasper, AL Bluegrass Community and Technical College, Lexington, KY Carolinas College of Health Sciences, Charlotte, NC Carteret Community College, Morehead City, NC Florida Gateway College, Lake City, FL George Corley Wallace State Community College, Selma, AL Huntingdon College, Montgomery, AL Jacksonville College, Jacksonville, TX Jefferson Community and Technical College, Louisville, KY Laredo College, Laredo, TX Midlands Technical College, Columbia, SC Mississippi Gulf Coast Community College, Perkinston, MS Mountain Empire Community College, Big Stone Gap, VA Panola College, Carthage, TX Pasco-Hernando State College, New Port Richey, FL Roane State Community College, Harriman, TN Robeson Community College, Lumberton, NC Southwest Mississippi Community College, Summit, MS Stillman College, Tuscaloosa, AL T.A. Lawson State Community College, Birmingham, AL Texas Southmost College, Brownsville, TX Texas State Technical College, Waco, TX Tri-County Community College, Murphy, NC Volunteer State Community College, Gallatin, TN Wade College, Dallas, TX The Board granted Candidacy status to the following institutions: Luther Rice College and Seminary, Inc., Lithonia, GA Northshore Technical Community College, Lacombe, LA 1 The Board reaffirmed the accreditation of the following institutions and requested a Monitoring Report: Cisco College, Cisco, TX Dillard University, New Orleans, LA Frank Phillips College, Borger, TX J. -

Friday, May 28, 2021-47Th Day (Cont.)
SENATE JOURNAL EIGHTY-SEVENTH LEGISLATURE Ð REGULAR SESSION AUSTIN, TEXAS PROCEEDINGS FORTY-SEVENTH DAY (Continued) (Friday, May 28, 2021) AFTER RECESS The Senate met at 11:46 a.m. and was called to order by the President. Senator Hughes offered the invocation as follows: Heavenly Father, we come before You and we just thank You for who You are. When we consider that You created everything, everything seen, everything unseen, we know that You existed before anything else, You always have and You always will. And, Father, we thank You for what we ve' learned, what we know about You. We know that You are all powerful, that You can do anything, nothing is in Your way, You can accomplish everything. We also know that You are all wise, You know exactly what You re' doing. You re' not caught by surprise by anything. You know exactly what s' happening. And, Father, we thank You that You are all loving. What You do is best, it s' best for us, even when we don t' understand. We thank You that we can trust You. And, Father, if we ever doubted Your love, we would just look at Calvary, where the Lord Jesus, Your Son, the creator, humbled Himself and there gave His life for us. The just for the unjust. We thank You for the resurrection, His ascension into heaven and His work there at Your right hand. Father, all these things we re' reminded You are for us in all these ways. In all these important ways these things that really matter. -

Special Meeting Agenda State of Texas )( City of Friendswood )( Counties of Galveston/Harris )( August 12, 2019 )(
SPECIAL MEETING AGENDA STATE OF TEXAS )( CITY OF FRIENDSWOOD )( COUNTIES OF GALVESTON/HARRIS )( AUGUST 12, 2019 )( NOTICE IS HEREBY GIVEN OF A SPECIAL MEETING OF THE FRIENDSWOOD CITY COUNCIL TO BE HELD ON MONDAY, AUGUST 12, 2019, AT 7:00 PM AT FRIENDSWOOD CITY HALL, COUNCIL CHAMBERS, 910 S. FRIENDSWOOD DRIVE, FRIENDSWOOD, TEXAS, TO DISCUSS THE ITEMS OF BUSINESS ACCORDING TO THE AGENDA LISTED BELOW: 1. Call to order 2. Invocation – Pastor Mike Ross, Friendswood Church of Christ 3. Pledge of Allegiance to the United States and Texas Flags – Cub Scouts Joseph Ford and Vincent Ford with Pack 452, Mary Queen (Honor the Texas flag; I pledge allegiance to thee, Texas, one state under God, one and indivisible) 4. Communications from the Public (To comply with provisions of the Open Meetings Act, the City Council may not deliberate on items discussed under this agenda item. The Council may refer this item to the City Manager or direct this item to be placed on the next regular Council agenda. PowerPoint presentations are not conducted during the citizen comment period. Out of respect for those speaking during public comment, please refrain from any outbursts or interjections to include, but not limited to, applause and/or disparaging noises from the audience. Doing so discourages others from voicing their thoughts and opinions, and disrupts the meeting.) 5. Discussion and possible action regarding approving a contract with Galveston County for Election Services. 6. Resolution Consideration and possible action regarding the following: A. Resolution R2019-25: A resolution of the City Council of the City of Friendswood, Texas, providing for the administration of a bond election. -

CITY of FRIENDSWOOD Notice of Public Hearings
CITY OF FRIENDSWOOD Notice of Public Hearings Notice of Public Hearings Regarding A Zone classification change request to replace Specific Use Permit (SUP) 98-22 with a revised SUP that will overlay all of the described properties which are zoned Single Family Residential (SFR) NOTICE is hereby given that the Planning and Zoning Commission and the City Council of the City of Fri endswood will each hold a public hearing to give all interested parti es the ri ght to appear and express their views on the fo ll owing item: • A zone classification change for approximately 54.805 acres known as Friendswood High School described as three tracts: 702/800 Greenbriar Dr. (main campus and sports fields) being a 39.177 acre tract of land located in the Sarah McKissick Survey, Abstract Number 151, City of Friendswood Galveston County, Texas and said 39.177 acre tract of land being the remainder of a called 41.558 acre tract described in the deed to Friendswood Independent School District recorded under Book 1835, Page 6 of the Galveston County Deed Records (GCDR); 1115 Falling Leaf Dr (natatorium) also known as Lot 1 Block 1 of the Final Plat of Friendswood High School Expansion, 7.788 acres being all of Lots 1 & 5 Brenham Estates (Volume 18, Page 601 , GCMR) and a portion of Lot 3, Block H Central Park Subdivision (Volume 15, Page 151, GCMR) Friendswood, Galveston County, Texas; and 1013 Falling Leaf Dr.; 1101 Falling Leaf Dr.; 0 Falling Leaf Dr.; 1014 Mustang Dr.; 1018 Mustang Dr.; 1102 Mustang Dr.; 1108 Mustang Dr. -

1:46.33 Rockwall High School 1 1:46.68 Friendswood High School 2
Lee & Joe Jamail Texas Swimming Center - Site License HY-TEK's MEET MANAGER 6.0 - 10:25 PM 2/4/2017 Page 1 2017 6A State Meet - 2/18/2017 Psych Sheet - 6A Prelims Event 1 Girls 200 Yard Medley Relay Team Relay Seed Time 1 Rockwall High School 1:46.33 2 Friendswood High School 1:46.68 3 Round Rock High School 1:46.85 4 Houston Stratford 1:47.20 5 Houston Westside 1:48.40 6 Austin Lake Travis 1:48.74 7 The Woodlands College Park 1:48.77 8 Keller High School 1:49.02 Event 2 Boys 200 Yard Medley Relay Team Relay Seed Time 1 Round Rock Westwood 1:34.61 2 Clear Falls High School 1:34.65 3 Round Rock McNeil 1:34.93 4 Houston Stratford 1:34.96 5 Lewisville Flower Mound 1:35.49 6 Friendswood High School 1:35.57 7 Cy-Fair Swim Team 1:35.64 8 Austin Vandegrift 1:35.94 Event 3 Girls 200 Yard Freestyle Name Year School Seed Time 1 Ashley Conrad 10 Rockwall-Heath 1:49.62 2 Morgan Johnson 11 Austin Westlake 1:50.60 3 Emma Hultquist 10 Rockwall High School 1:50.68 4 Sutton Marvin 12 Round Rock McNeil 1:51.27 5 Rachel Hicks 11 Atascocita High School 1:51.35 6 Samantha Howell 12 Austin Lake Travis 1:51.44 7 Halle Gordon 10 Austin Westlake 1:51.99 8 Sammie Antonacci 12 San Antonio Reagan 1:52.29 Event 4 Boys 200 Yard Freestyle Name Year School Seed Time 1 Jack Dunworth 12 Austin Westlake 1:40.30 2 Will Thomas 12 Austin Westlake 1:40.90 3 Christian Weispfennig 09 Glenda Dawson High School 1:40.93 4 Kevin Repice 10 Southlake Carroll 1:41.00 5 Jacob Powell 10 Klein High School 1:41.27 6 Christian Rossi 12 Cinco Ranch High School 1:41.35 7 Luke Stuart 11 Montgomery -

WEB STATS REPORT: January Texas TOP 20 21
WEB STATS REPORT: January Texas TOP 20 21. Pleasanton High School 12416 56. San Angelo Central High School 4533 22. Everman High School 12045 57. L C Anderson High School 4233 1. Temple High School 125449 23. Denton High School 11932 58. Sherman High School 4213 24. Elgin High School 11658 59. Natalia High School 4197 2. Belton High School 59420 25. Magnolia West High School 11517 60. Centennial High School 4141 3. Calhoun High School 44650 26. Life School Waxahachie 11216 61. John Foster Dulles High School 4120 27. Highland Park High School 10432 62. Grapevine High School 4071 4. Lovejoy High School 25514 28. Ennis High School 10257 63. Clear Brook High School 4058 29. Cinco Ranch High School 9204 64. Haskell High School 4005 5. Southlake Carroll HS 24391 30. Stephen F Austin High School 9173 65. Cypress Ridge High School 3940 6. Midway High School 22547 31. Salado High School 9142 66. Cypress Springs High School 3851 32. Life School Oak Cliff HS 8342 67. Pearland High School 3685 7. Forney High School 19580 33. Burleson High School 7932 68. Goose Creek Memorial HS 3677 34. Midland Lee High School 7908 69. Clark High School 3669 8. Magnolia High School 17382 35. Westfield High School 7902 70. Daingerfield High School 3660 9. Hays High School 16848 36. San Antonio Christian HS 7874 71. Lutheran High School 3618 37. Andy Dekaney High School 7834 72. Great Hearts Northern Oaks 3581 10. North Forney High School 16706 38. North Crowley High School 7602 73. Edcouch-Elsa High School 3513 39. -

(713) 525-3500 Or Admiss
Find the school district in which your Houston high school is located. For Private high schools, search for your school under the "Private" heading. If you are unable to determine your UST Admissions Couselor, please contact the Office of Admissions at (713) 525-3500 or [email protected] Aldine Independent School District Aldine Senior High School Arthur Ortiz [email protected] 713-525-3848 Eisenhower High School Arthur Ortiz [email protected] 713-525-3848 H P Carter Career Center Arthur Ortiz [email protected] 713-525-3848 J. L. Anderson Academy Arthur Ortiz [email protected] 713-525-3848 MacArthur High School Arthur Ortiz [email protected] 713-525-3848 Nimitz High School Arthur Ortiz [email protected] 713-525-3848 Victory Early College HS Arthur Ortiz [email protected] 713-525-3848 W T Hall High School Arthur Ortiz [email protected] 713-525-3848 G W Carver High School Arthur Ortiz [email protected] 713-525-3848 Aleif Independent School District Alief Hasting Senior High Sch Goli Ardekani [email protected] 713-942-3468 Alief Taylor High School Goli Ardekani [email protected] 713-942-3468 Elsik High School Goli Ardekani [email protected] 713-942-3468 Kerr High School Arthur Ortiz [email protected] 713-525-3848 Alvin Independent School District Alvin High School Goli Ardekani [email protected] 713-942-3468 Manvel Goli Ardekani [email protected] 713-942-3468 Anahuac Independent School District Anahuac High School Mi'Chelle Bonnette [email protected] 713-942-3475 Angleton Independent School District Angleton High School Mi'Chelle Bonnette