TARA SHAH Prof
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Study Report on "Comminity Based Organizations(Cbos): Landscape
Community Based Organizations (CBOs): Landscape, Capacity Assessment and Strengthening Strategy Study Report Prepared for PLAN Nepal Lalitpur, Nepal July, 2005 Democratizing civil society at grassroots SAGUN P.O. Box 7802, Kathmandu, Nepal Phone: 977 4247920, Fax: 9771 4229544 Email: [email protected] Community Based Organizations (CBOs): Landscape, Capacity Assessment and Strengthening Strategy Mukta S. Lama Suresh Dhakal Lagan Rai Study Report Prepared for PLAN Nepal Lalitpur, Nepal July, 2005 SAGUN P.O. Box 7802, Kathmandu, Nepal Phone: 977 4247920, Fax: 9771 4229544 Email: [email protected] ii Acknowledgements This report is a result of contribution of many people in multiple ways. Foremost, we extend our deepest and heartfelt gratitude to members of Community Based Organizations across the districts for sharing us with their time, insight and experiences. The study benefited greatly from support and cooperation of the Plan field staff and partner agencies in Sunsari, Morang, Makwanpur, Rautahat, Bara, and Banke districts and the Regional Operational Support Unit teams. We would like to thank Ms. Chhing Lamu Sherpa, Mr. Kalbhan Rai, Dr. Chandra K. Sen, Mr. R. P. Gupta and Krishna Ghimire for their valuable inputs on the study. Dr. Chandi Chapagai, Plan Nepal Country Training Coordinator deserves special thanks for coordinating the whole exercise. We would like to express our deep appreciation to Shobhakar Vaidhya for his keen interest, insightful comments and his enthusiasm for incorporating the learning into the institutional policies and procedures. Thanks are also due to the Ms. Minty Pande, Country Director for her encouragement and comments. Similarly we very much appreciate the support of Mr. -

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -
Existing Environmental Conditions
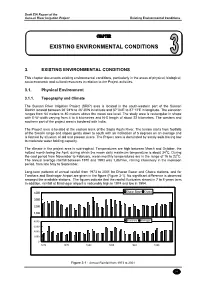
Draft EIA Report of the Sunsari River Irrigation Project Existing Environmental Conditions CHAPTER EXISTING ENVIRONMENTAL CONDITIONS 3. EXISTING ENVIRONMENTAL CONDITIONS This chapter documents existing environmental conditions, particularly in the areas of physical, biological, socio-economic and cultural resources in relation to the Project activities. 3.1. Physical Environment 3.1.1. Topography and Climate The Sunsari River Irrigation Project (SRIP) area is located in the south-western part of the Sunsari District located between 26°24′N to 26°30′N in latitude and 87°04′E to 87°12′E in longitude. The elevation ranges from 64 meters to 80 meters above the mean sea level. The study area is rectangular in shape with E-W width varying from 4 to 8 kilometres and N-S length of about 22 kilometres. The western and southern part of the project area is bordered with India. The Project area is located at the eastern bank of the Sapta Koshi River. The terrain starts from foothills of the Siwalik range and slopes gently down to south with an inclination of 5 degrees on an average and is formed by alluvium of old and present rivers. The Project area is dominated by sandy soils having low to moderate water holding capacity. The climate in the project area is sub-tropical. Temperatures are high between March and October, the hottest month being the April, during which the mean daily maximum temperature is about 340C. During the cool period from November to February, mean monthly temperatures are in the range of 16 to 220C. The annual average rainfall between 1970 and 1993 was 1,867mm, raining intensively in the monsoon period, from late May to September. -

Ltzt Ul/Alsf Ljifdtf -K
1 2 lhNnfx?sf] ul/aLsf] b/, ul/aLsf] ljifdtf / ul/aLsf] uxgtf @)^* lhNnf uf=lj=;=sf gfd ul/aLsf b/ ul/aLsf ljifdtf ul/aLsf uxgtf -k|ltzt_ -k|ltzt_ -k|ltzt_ ;'g;/L k+rsGof 4.66(2.39) 0.63(0.39) 0.14(0.1) ;'g;/L lj:g'kfb'sf 11.25(6.3) 1.76(1.21) 0.44(0.35) ;'g;/L j/fxIf]q 5.08(2.33) 0.72(0.39) 0.17(0.1) ;'g;/L dx]Gb|gu/ 10.43(4.6) 1.89(1.02) 0.53(0.33) ;'g;/L jSnf}/ 9.59(5.29) 1.54(1.06) 0.39(0.32) ;'g;/L d/f}n 7.48(3.03) 1.1(0.55) 0.26(0.15) ;'g;/L x+f;kf];f 4.09(1.81) 0.6(0.31) 0.14(0.08) ;'g;/L vgf/ 4.52(1.95) 0.66(0.34) 0.15(0.09) ;'g;/L dw]nL 9.02(4.58) 1.55(0.98) 0.42(0.31) ;'g;/L l;dl/of, tgd'gf 15.73(4.92) 2.97(1.2) 0.85(0.41) ;'g;/L ;f]gfk'/ 13.63(5.98) 2.67(1.5) 0.8(0.53) ;'g;/L b'xjL, en'jf 9.11(3.98) 1.6(0.89) 0.44(0.29) ;'g;/L k'j{s'zfxf, l56fxf 18.27(5.66) 3.54(1.42) 1.04(0.5) ;'g;/L /fhu+h a]nufl5of, cd8'jf 18.18(4.91) 3.42(1.21) 0.98(0.41) ;'g;/L cdflxa]nf, lrd8L 15.26(5) 2.86(1.19) 0.82(0.4) ;'g;/L PsDaf 6.93(2.73) 1.13(0.53) 0.29(0.16) ;'g;/L efbufFp l;g'jf/L 4.77(2.46) 0.77(0.48) 0.2(0.14) ;'g;/L rfFbj]nf 12.07(5.79) 2.11(1.27) 0.57(0.4) ;'g;/L ksnL 6.23(3.35) 0.99(0.64) 0.25(0.19) ;'g;/L l;+luof 9.55(5.08) 1.57(1.03) 0.4(0.31) ;'g;/L alaof 15.92(6.76) 2.89(1.56) 0.8(0.51) ;'g;/L hNkfk'/ 22.98(9.23) 4.29(2.26) 1.21(0.76) ;'g;/L dw];f 6.29(3.63) 1.02(0.73) 0.26(0.22) ;'g;/L cf}/fjgL 11.35(5.46) 2.04(1.21) 0.57(0.39) ;'g;/L uf}tdk'/ 13.11(6.39) 2.28(1.4) 0.62(0.45) ;'g;/L ;Q]/em]f/f, /fhu+h l;g'jf/L 22.54(6.83) 4.45(1.8) 1.32(0.65) ;'g;/L dWoxiff{xL, b]jfgu+h 15.52(5.27) 2.74(1.19) 0.75(0.38) ;'g;/L sKtfgu+h, ;fx]au+h 17.45(5.69) -

Plan International USA, Inc. D/B/A Plan USA ______
Plan International USA, Inc. d/b/a Plan USA _____________________________________ Local Innovation for Better Outcomes for Neonates Project (LIBON) Sunsari, Parsa and Bara Districts of Nepal Plan Nepal Child Survival Project XXII Cooperative Agreement No. GHN-A-00-07-00006-00 30 September 2007 – 29 September 2011 2nd Annual Report (October 1, 2008 - Sept 30, 2009) Report Submitted: October 30, 2009 Report Prepared by: Bhagawan Das Shrestha – Project Coordinator/LIBON Dipak Dahal – Monitoring and Evaluation Officer/LIBON With Support from: Kalawati Changbang - HPC and DLC Sunsari Hari Dev Shah – ADLC Sunsari Deo Ratna Chaudhary – DLC Bara/Parsa Krishna Bahadur Achhami – ADLC Parsa Diwakar Mishra – ADLC Bara Meena Kumari Singh – Administrative and Finance Assistant ACRONYMS ADLC - Assistant District LIBON Coordinator AHW - Auxiliary Health Worker (HP, SHP) ANC - Antenatal Care ANM - Auxiliary Nurse Midwife ARI - Acute Respiratory Infection BCC - Behavior Change Communication CATCH - Core Assessment Tool for Child Health CB-NCP - Community Based – Newborn Care Program CBO - Community Based Organization CHD - Child Health Division, Ministry of Health and Population CHX - Chlorhexidine CSSA - Child Survival Sustainability Assessment CSTS - Child Survival Technical Support DDC - District Development Committee DEO - District Education Office DHO - District Health Office DIP - Detailed Implementation Plan DLC - District LIBON Coordinator DoHS - Department of Health Service, MoHP DPHO - District Public Health Office DTOT - District Training of -

Pdf | 808.65 Kb
Koshi River Flood (Nepal): Emergency Areas Declared by the Government of Nepal ( Sept.5, 2008) 86°52'30"E 87°0'0"E 87°7'30"E 87°15'0"E Phattehapur Tapeshworibelahi Bakloura Odraha Mahendranagar Bakloura Udayapur On September 5, the Government of Nepal has Sundarpur Kamalpur Singiya declared state of emergencyHansposa in Kusahapaschim, R Shreehariipur, Shreepurjavdi, Lokhahi, Madhuban, E Prakashpur IV Narshingha, Bokraha,Pakali Ramnagar Bhutaha, R Dhodhanpur I Basantapur, Dhuskee VDCs and Inaruwa Muncipality H S of Sunsari district and Bhardaha VDc of Saptari O Itahari Municipality K District. A Bhadgaun Sinuwari T P Roopnagar A Koshi Tappu Wildlife Reserve S Dharampur Dharampur Dulari Pipra (Purba) Koshi Tappu Wildlife Reserve Dumraha BakdhuwaMap Locator Madhuban Ekamba Dharampur 050 100Theleya 200 300 Kilometers Kanchanpur Madhesa Khanar Jagatpur Bhokraha 26°37'30"N Legend Embankment Breach Point Boundaries Chandbela [ Kusahapaschim 26°37'30"N District Badgama Madhali VDC N E P A L Major Roads Inarwa Municipality Baramjhiya LohajaraHighway Sonapur Sisbani Badhara Feeder Road Menakadari District Road Lokahi Other Road Saptari Dangraha Water bodies Badgama Parashbani Emergency Areas Aurabani Trikaul Duhavi Declared Area Bairawa Babiyabirta Simaria Demon Goethi Narshigha Sunsari Paurataha Shreepurjavdi Hathimudha Dadha Trikaul Jalpapur Satterjhora Tanmuna Madhuwapur Bhardaha Bhaluwa Bhagawatpur KOSHI BARRAGE Joginiya-2 Shreeharipur Ramnagar Bhutaha Chhitaha Tankisinuwari Mahadewa Bathanaha Joginiya-1 Gautampur Joginiya-2 Morang Purba Kusahha -

Integrated Or Isolated? How State and Non-State Justice Systems Work for Justice in Nepal District Assessment Report
INTEGRATED OR ISOLATED? How state and non-state justice systems work for justice in Nepal District assessment report May 2012 b International Alert About International Alert International Alert is a 26-year-old independent peacebuilding organisation. We work with people who are directly affected by violent conflict to improve their prospects of peace. And we seek to influence the policies and ways of working of governments, international organisations like the UN and multinational companies, to reduce conflict risk and increase the prospects of peace. We work in Africa, several parts of Asia, the South Caucasus, the Middle East and Latin America, and have recently started work in the UK. Our policy work focuses on several key themes that influence prospects for peace and security – the economy, climate change, gender, the role of international institutions, the impact of development aid, and the effect of good and bad governance. We are one of the world’s leading peacebuilding NGOs with more than 159 staff based in London and 14 field offices. To learn more about how and where we work, visit www.international-alert.org. The Consortium Partners About Forum for Women, Law and Development (FWLD) Forum for Women, Law and Development (FWLD) (partner) was founded in 1995 with the aim of protecting and promoting women’s human rights enshrined within CEDAW. To this end, FWLD’s work focuses largely on the implementation of international instruments protecting these rights, such as UNSCR 1325. Main activities include research into the legal status of Nepali women, rights-based advocacy, public interest litigation, public education, media campaigning and training. -

The Feasibility Study on the Sunsari River Irrigation Project in the Kingdom of Nepal
JAPAN INTERNATIONAL COOPERATION AGENCY (JICA) DEPARTMENT OF IRRIGATION MINISTRY OF WATER RESOURCES HIS MAJESTY’S GOVERNMENT OF NEPAL THE FEASIBILITY STUDY ON THE SUNSARI RIVER IRRIGATION PROJECT IN THE KINGDOM OF NEPAL FINAL REPORT APPENDIXES January, 2003 SANYU CONSULTANTS INC. AFA JR 03-05 CONTENTS APPENDIXES APPENDIX-1 SCOPE OF WORK, MMs AND CONCERNED OFFICERS APPENDIX-2 REGIONAL ECONOMY APPENDIX-3 RURAL SOCIOLOGY AND GENDER APPENDIX-4 METEOROLOGY, HYDROLOGY AND HYDRO-ANALYSIS APPENDIX-5 AGRICULTURE DEVELOPMENT APPENDIX-6 IRRIGATION AND DRAINAGE DEVELOPMENT APPENDIX-7 HYDRO-GEOLOGY AND GROUNDWATER DEVELOPMENT APPENDIX-8 IRRIGATION FACILITIES AND RURAL INFRASTRUCTURE APPENDIX-9 INSTITUTIONAL DEVELOPMENT APPENDIX-10 ENVIRONMENT APPENDIX-11 COST RECOVERY AND PROJECT EVALUATION APPENDIX-12 PROJECT COST ACRONYMS AND ABBREVIATIONS ADB Asian Development Bank ADBN Agriculture Development Bank of Nepal ADO Agriculture Development Officer AIC Agricultural Inputs Corporation AO Association Organizer (employed by SMIP) APP Agricultural Perspective Plan AREP Agricultural Research and Extension Project (WB funded) ASC Agriculture Service Center CBS Central Bureau of Statistics CDO Chief District Officer CE Collection Efficiency (of Irrigation Service Fee) CMC Chatra Main Canal EDR Eastern Development Region ERID Eastern Regional Irrigation Directorate CGWISP Community Groundwater Irrigation Sector Project (ADB funded) DAC District Agriculture Committee DADO District Agricultural Development Office DDC District Development Committee DIO District -
Impact Evaluation of Sunsari-Morang Irrigation Project
Final Report National Planning Commission Secretariat M &E Division, SMES 2 Singha Durbar, Kathmandu Impact Evaluation of Sunsari-Morang Irrigation Project Submitted by Project Research and Engineering Associates Lagankhel, Lalitpur December, 2012 Contents Preface Summary 1. Introduction ......................................................................................................................................... 1.1 Background of the Evaluation......................................................................................................... 1 1.2 Objective of the Impact Evaluation..................................................................................................3 1.3 Description of Evaluators ……………………………………....................................................... 4 1.4 Approach and Methodology of Impact Evaluation......................................................................... 4 -Qualitative Method -Quantitative Method -Triangulation Method 2. Basic Information of Sunsari Morang IrrigationProject .................................................................. 16 2.1 Background of SMIP ..................................................................................................................... 16 2.2 Objectives of SMIP........................................................................................................................18 2.3 Description of SMIP ...................................................................................................................... 18 2.4 -

Download CSDC Profile
Organizational Profile Community for Social Development Centre (CSDC) March, 2021 Community for Social Development Center (CSDC) Organizational Profile 1 1. Introduction Name: Community for Social Development Center (CSDC) Established: 5th Feb, 2000 A.D. (2056.10.22 B.S.) Type of Organization: NGO (Social Development Organization) Centre Office: Dewanganj-1, Sunsari Sunsari Dist. office: Inaruwa-5, in front of DAO office Sunsari, PH# 025-620688 Regional/ Head Operation office: Biratnagar -11, Behind Nepal Bajar Web: www.csdc.org.np Email: [email protected], Contact Person: Mr. Indra Kumar Karn [email protected] Designation: Chairperson Mobile: 9807350216/ 9852057790 2. Registration and Affiliation th District Admin. Office, Sunsari Reg No.–727/692/056/057- 16 March, 2000 (2056.12.3 B.S.) District admin office, Morang Ref. No.- 1245/066/67- 15th Sep, 2009 (2066/05/30 BS) District administration office, Banke Ref No. : 6410/068/069 - 7th May, 2012 (2069/01/25 BS) Social Welfare Council, Nepal, Reg No. -11618/057 - 21st Dec, 2000 (2057.09.06 B.S.) Social Welfare council, Nepal Renewed on 2073/11/09 for 2076/03/31 (3 years) Non-Govt. organization Coordination Committee, Sunsari - 2000 A.D. NGO Federation, Sunsari - 2007 A.D. District Development Committee Internal Revenue office, Dharan PAN/ No: 302874729 - 2008 A.D. Internal Revenue office, Itahari PAN /VAT/ No: 302874729 - 2069/ 09/22 BS Time period of Board of Directors – 2 Years Last date of General Assembly 2077/ 09/ 25 BS (09 JAN, 2021) Last date of Organizational Renewed, 2077/ 10/ 23 BS (05 FEB, 2021) Community for Social Development Center (CSDC) Organizational Profile 2 VMGOs: Vision: To establish an innovative and impartial society by gradual development of rural and backward communities. -

Fb C/Ljgb S"Df/ /Fpt आडिल कुमारी गुप्ता जगन्नाथ स
खुला प्रलतयोलगता配मक परीक्षाको वीकृ त नामावली वबज्ञापन नं. : २०७७/७८/२१ (प्रदेश नं. २) तह : ४ पदः सहायक रोल नं. उ륍मेदवारको नाम उ륍मेदवारको नाम ललंग सम्륍मललत हुन चाहेको समूह थायी म्ि쥍ला थायी न. पा. / गा.वव.स बािेको नाम बाबुको नाम 1 AACHAL RAUT cf+rn /fpt Female ख쥍ु ला, महिला, मधेशी Bara Nijgadh hgswf/L k|;fb c/ljGb s"df/ /fpt 2 AADALI KUMARI GUPTA आडिल कु मारी गुप्ता Female ख쥍ु ला, महिला, मधेशी Dhanusa Janakpur जगन्नाथ साह डिजय साह 3 AAISHA KHATOON cfO;f vft"g Female ख쥍ु ला, महिला, मधेशी Dhanusa Tarapatti Sirsiya dxdb cf]lndg dxdb /lkms 4 AAKASH KUMAR JHA cfsfz s"""df/ ‰mf Male ख쥍ु ला, मधेशी Dhanusa janakpurdham k"/Gb/ ‰mf clg?$ ‰mf 5 AAKRITI NIDHI आकृ डि डिडि Female ख쥍ु ला, महिला Dhanusa Janakpur हररिाथ डिडि सडु िल कु मार डिडि 6 AANAND KUMAR YADAV cfgGb s"df/ ofbj Male ख쥍ु ला, मधेशी Siraha Pipra Pra Pi d"lgnfn ofba dxfb]j ofbj 7 AARADHNA CHAUDHARY अराििा चौिरी Female ख쥍ु ला, महिला, मधेशी Mahottari Jaleshwar शभु करण चौिरी श्याम डकशोर चौिरी 8 AARATI KARN आरिी कणण Female ख쥍ु ला, महिला, मधेशी Dhanusa Tarapatti Sirsiya प्रमोद लाल कणण डिरेन्द्र लाल कण ण कायस्थ 9 AARTI CHAUDHARY आरिी चौिरी Female ख쥍ु ला, महिला, आहिवासी / जनजाति Bara Baragadi टुगर चौिरी zf]ef चौिरी 10 AARTI GIRI cf/lt lul/ Female ख쥍ु ला, महिला Dhanusa chhireswarnath v*\u axfb"/ lu/L kf]i^ axfb"/ lu/L 11 AARTI GUPTA आरिी गुप्ता Female ख쥍ु ला, महिला Parsa sabaithawa गौरी प्रसाद गुप्ता सरु ेश कु मार गुप्ता 12 AARTI KUMARI JHA cf/tL s'df/L emf Female ख쥍ु ला, महिला Dhanusa Laxmipur Bageba afn s[ifण emf OGb| gf/fo)f emf 13 AARTI KUMARI SHRESTHA cf/lt s"df/L >]i& Female ख쥍ु ला, महिला, -

District Transport Master Plan (DTMP) for Sunsari District ------Acknowledgements
Government of Nepal District Transport Master Plan (DTMP) For Sunsari District Ministry of Federal Affairs and Local Development Department of Local Infrastructure Development and Agricultural Roads (DoLIDAR) District Development Committee, Sunsari Final Report Volume I: Main Report 2013 Prepared by the MULTI Disciplinary Consultants (P) Ltd for the District Development Committee (DDC) and District Technical Office (DTO), Sunsari with Technical Assistance from the Department of Local Infrastructure and Agricultural Roads (DoLIDAR) Ministry of Federal Affairs and Local Development and grant supported by DFID. District Transport Master Plan (DTMP) For Sunsari District ------------------------------------------------------------------------------------------------------------------------------------------------ Acknowledgements MULTI Disciplinary Consultants (P) Ltd. take great pleasure to express the deepest gratitude to the District Development Committee, Sunsari GoN / DoLIDAR/RTI for intrusting us to carry out preparing of this District Transport Master Plan (DTMP) of Sunsari District. We would like to express our deep gratitude to Mr. Rajendra Dev Pandey / LDO, Sunsari , Mr. Krishna Kumar Mishra /DTO, DDC staffs, all party representatives, all VDC secretaries, all the people of Sundari including dalit, women and Janajati who had contributed to the project for all cooperation and help rendered in the pursuit of our work. We also appreciate the valuable suggestion relevant technical information and cooperation provided by LDO, CDO all political party members of Sunsari District, Engineer from DTO, VDC secretaries of 48 VDCs, Ex – VDC Chairman and all participants of workshop during the project period. Deep insight have gone for quality outputs of preparing DTMP of Sunsari District taking into considerations of constraints of topography, accessibility and other factors. Therefore we also like to acknowledge Team Leader, Technical team, GIS Expert and Civil Engineers who have contributed to achieve it.