Fall 2016 Updates Create Service Improvements Alison Lacarrubba, DVM, DABVP
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2006 NC State 4-H Hippology Contest
2006 NC State 4-H Hippology Contest Senior Division Ids Answers are in red. 1. Identify this breed. A. Arabian B. Hackney C. Morgan D. Saddlebred 2. Identify the color of this horse. A. Blue roan B. Dappled grey C. Flea-bitten grey D. Grulla 3. Identify this face marking. A. Bald Face B. Blaze C. Star D. Stripe 4. What is the name for the item this horse is wearing on its head? A. Blinders B. Blinkers C. Face Mask D. Fly Mask 5. The yellow arrows are pointing to a leg joint, which one? A. Hip Joint B. Hock Joint C. Pelvis D. Stifle Joint 6. Identify this coat pattern. A. Overo B. Pinto C. Tobiano D. Tovero 7. Identify this roughage. A. Alfalfa B. Bermuda Grass C. Fescue D. Orchardgrass 8. Identify this piece of hardware. A. Bridle Rack B. Clothes Rack C. Coat Rack D. None of the Above 9. Identify this piece of tack. A. Action Device B. English Curb Chain C. Rounders D. Western Curb Chain 10. Identify this high energy grain. A. Barley B. Milo C. Oats D. Rye 11. From what disease condition is his horse suffering? Swollen lymph glands that may burst A. Equine Viral Arteritis B. Equine Viral Rhinopheumonitis C. Influenza Pus discharge from nostrils D. Strangles 12. Identify this bit. A. Dr. Bristol B. Eggbutt Ring Snaffle C. Loose Ring Bradoon D. Pelham 13. This paint coat pattern is typically a _______ genetic trait. A. dominant B. mutant C. recessive D. trisomy 14. You are viewing the front feet of one horse. -

Read Book Through England on a Side-Saddle Ebook, Epub
THROUGH ENGLAND ON A SIDE-SADDLE PDF, EPUB, EBOOK Celia Fiennes | 96 pages | 02 Apr 2009 | Penguin Books Ltd | 9780141191072 | English | London, United Kingdom Sidesaddle - Wikipedia Ninth century depictions show a small footrest, or planchette added to the pillion. In Europe , the sidesaddle developed in part because of cultural norms which considered it unbecoming for a woman to straddle a horse while riding. This was initially conceived as a way to protect the hymen of aristocratic girls, and thus the appearance of their being virgins. However, women did ride horses and needed to be able to control their own horses, so there was a need for a saddle designed to allow control of the horse and modesty for the rider. The earliest functional "sidesaddle" was credited to Anne of Bohemia — The design made it difficult for a woman to both stay on and use the reins to control the horse, so the animal was usually led by another rider, sitting astride. The insecure design of the early sidesaddle also contributed to the popularity of the Palfrey , a smaller horse with smooth ambling gaits, as a suitable mount for women. A more practical design, developed in the 16th century, has been attributed to Catherine de' Medici. In her design, the rider sat facing forward, hooking her right leg around the pommel of the saddle with a horn added to the near side of the saddle to secure the rider's right knee. The footrest was replaced with a "slipper stirrup ", a leather-covered stirrup iron into which the rider's left foot was placed. -
Pre-Ride Checklist with BONUS Pre-Show Checklist
Pre-Ride Checklist with BONUS Pre-Show Checklist Pre-Ride Checklist: Why? A few simple checks BEFORE you ride can protect your horse from injury and save your time and money. A well-used pre-ride checklist will minimize the chance of an accident to horse and rider and maximize your valuable lesson time (= $$). When you and your horse are ready to ride, physically and mentally, in safe and quality tack, before your lesson starts, you don’t waste your, your trainer and your horse’s time/energy. You don’t waste your money as your lesson ticks away while you are looking for your spurs while the rest of the group just jumped the big oxer in the outdoor arena. At Swan Training we recommend a simple yes/no checklist modeled on the USPC inspection list with a few of our own values added. We hope you print it, keep in your tack trunk, and use it before every ride. Pre Ride Checklist YES NO NOTES RIDER Safe, neat & clean attire Appropriate attire for the event Boots in good repair, appropriately clean Spurs (if used) put on properly; polished HORSE (the rider preforms the horse pre- checks before mounting, regardless of who was responsible for preparing the horse) Well groomed, reflecting regular care; no sweat marks or dirt; healthy coat Mane and tail clean and tangle-free Sheath/udder showing regular care Feet well-trimmed and/or shod Feet picked out Eyes, nose, lips, dock clean TACK Safe, clean, supple, reflecting regular care Properly adjusted All stress points clean No cracked leather Metal clean & polished No residue in holes or lacings Saddle pad clean & brushed Tighten girth before and after mounting SPORTSMANSHIP Mentally ready to ride Ready to work in sportsmen-like manner with trainers and barn mates Physically prepared to work PRE-RIDE CHECKLIST (EQUI SUPERMARKET 2017) 1. -

Lawrie & Symington Ltd Forfar Mart MONDAY 6 MAY 2019
Lawrie & Symington Ltd Forfar Mart MONDAY 6th MAY 2019 ‘MAY DAY’ SALE OF TACK, HORSE BOXES, CARTS & TRAILERS ALL ITEMS SUBJECT TO ARRIVAL Sale to commence at 10.30 am with Tack in The Strathmore Hall Followed by Trailers, Horse Boxes & Carts Buyer’s premium of 10% will be added to purchaser bills + VAT at 20% on the 10% commission ONLY CATALOGUE £2.00 Tack to commence at 10.30 am in THE STRATHMORE HALL Followed by Trailers & Carts OUTSIDE TACK WILL NOT BE ACCEPTED ON THE DAY OF SALE ALL INTENDING PURCHASERS ARE TO SATISFY THEMSELVES AS TO WHAT IT IS THEY ARE PURCHASING EACH LOT BECOMES THE SOLE RESPONSIBILITY OF THE PURCHASER AT THE FALL OF THE HAMMER FORFAR MART TAKES NO RESPONSIBILITY FOR DESCRIPTIONS GIVEN TACK ITEMS 1 STALLION SHOW ROLLER, LEATHER NEW 2 IN HAND LEATHER/BRASS SHOWING BRIDLE 3 SADDLE RAISER PAD, NEW JOHN WHITTAKER, NAVY, RED/WHITE TRIM 4 GRAZING MUZZLE, ADJUSTABLE, PONY SIZE, BLUE 5 QUILTED WEATHERBETA JASPER STABLE RUG 5’6” BLUE 6 SADDLE, THOROWGOOD, BLACK 7 WATER CONTAINER/JUMP PROP, WARHORSE, PURPLE 30L 8 CLIPPERS, ELECTRIC, LIVERYMAN WITH CASE 9 BE-NICE CONTROL HALTER, AS NEW, RUBY/GRASS PONY SIZE 10 DUBLIN SHOWING JACKET 11 AIGLE GILET SIZE 12/14 NAVY/CREAM 12 FLYDEX STABLE SPRAY WITH VIRBAC APPLICATOR GUN 13 JACK MURPHY SEAL 3000 SALMON OUTDOOR JACKET SIZE 12 14 CRANE EQUESTRIAN MINK/PINK FLEECE PULLOVER MED 12/14 15 RIDING BOOTS SIZE 5, AS NEW. HUNTER BOOT BAG 16 NUPOWER VEHICLE CHARGER/STARTER WITH BOX 17 LAMBSKIN GRACKLE FLUFF, NEW – SEW ON 18 WEBBING HEAD COLLAR NEW, GRAZING MUZZLE, BLACK 19 LEATHER SADDLE, -

National Gear Rules
NATIONAL GEAR RULES Effective from January 1, 2022 Published by Pony Club Australia Ltd ABN 95 090 080 265 www.ponyclubaustralia.com.au This publication can be downloaded for Pony Club purposes Contents Introduction .......................................................................................................................................................................... 6 Complying with the rules .................................................................................................................................................. 7 Gear Exemption Forms ..................................................................................................................................................... 7 Disciplines Covered in The National Gear Rules ................................................................................................................... 8 Definition of Formal, Informal and Open Rider Attire ........................................................................................................ 10 Section 1: Rider Attire ..................................................................................................................................................... 11 1.01 Air vests ............................................................................................................................................................... 11 1.02 Badges ................................................................................................................................................................ -
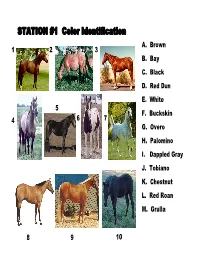
STATION #1 Color Identification A
STATION #1 Color Identification A. Brown 12 3 B. Bay C. Black D. Red Dun E. White 5 F. Buckskin 4 67 G. Overo H. Palomino I. Dappled Gray J. Tobiano K. Chestnut L. Red Roan M. Grulla 89 10 STATION #2 Markings 12 34 A. Ankle B. Blaze C. Coronet D. Distal spots 67 E. Freckles F. Bald face 5 G. Half stocking H. Full stocking I. Snip J. Pastern K. Mottled skin L. Star 8910 STATION #3 Parts of Hoof & Lower Leg 1 2 3 A. Short Pastern B. Frog C. Sesamoid D. Wall 6 E. Bar F. Cannon 4 G. Navicular 5 7 H. Sole I. White line 8 10 J. Coffin K. Laminae 9 L. Long pastern STATION #4 WESTERN SADDLE PARTS 2 3 A. Stirrup 4 B. Skirt 1 C. Seat Jockey 5 D. Pommel E. Keeper F. Horn 10 6 G. Back Cinch Strap H. Fender 7 I. Seat 8 J. Latigo Strap K. Cantle 9 STATION #5 Uses And Events 123A. Cutting B. Barrel Racing C. Polo D. Fox Hunting E. Showmanship 45 6 F. Jumping G. Reining H. Trail Riding I. Team Penning J. Bareback Bronc Riding K. Calf Roping 78910 STATION #6 Parasite Identification 1 234 A. Horse fly B. Deer fly C. Mange mite D. Strongyles E. Ascarids 567 F. Mosquito G. Deer tick H. Bot fly I. Stable fly J. Bot larva K. Lice 89 10 STATION #7 TACK IDENTIFICATION A. Shipping boots 1 B. Body brush 2 C. War bridle 3 D. Fly mask E. Blinkers F. Splint boots 6 G. -

Horse Vaccines
Western Ranch Supply “Serving the Big Country” ORDER ONLINE www.westernranchsupply.com FALL 2018 BUYING GUIDE Billings: (406) 252-6692 PHONE (800) 548-7270 TOLL FREE Great Falls: (406) 761-2160 PHONE (800) 548-5855 TOLL FREE Your locally owned & operated Western“Serving Ranch The Big Country” Supply Farm & Ranch Supply store NOWNOW ONLINEONLINE WWW.WESTERNRANCHSUPPLY.COMWWW.WESTERNRANCHSUPPLY.COM Clothing | Footwear | Home Decor We Livestock Handling Equipment | Automotive Hardware & Tools | Tack Handle: Animal Health Products Free delivery in Montana & Wyoming (some exclusions may apply) WEST END LOCATION: 7305 ENTRYWAY DRIVE • BILLINGS, MT 59101 TH DOWNTOWN LOCATION: 303 NORTH 13 STREET • BILLINGS, MT 59101 406-252-6692 • 800-548-7270 GREAT FALLS LOCATION: 4000 RIVER DRIVE NORTH • GREAT FALLS, MT 59401 • 800-548-5855 • 406-761-2160 VISIT OUR STORES! * 7305 Entryway Drive, Billings, Montana Open Monday-Saturday: 8am-6pm, CLOSED Sunday Billings Metra Park * 1st Ave North 303 North 13th Street - Billings, Montana *NEW HOURS* Open Monday-Friday: 8am-5pm, CLOSED Saturday & Sunday Shop Address: 1615 Sixth Ave North - Billings, MT. 59101 North* Star Blvd 38th St N St 38th 4000 River Drive North - Great Falls, Montana Open Monday-Saturday: 8am-5pm, CLOSED Sunday COVER PHOTO BY: Amy Thompson (Moore, Montana) Order by Phone: ORDER ONLINE! Social Media 1-800-548-7270 www.westernranchsupply.com Billings, MT 1-800-548-5855 NEW PRODUCTS ADDED Great Falls, MT DAILY! Orders should be called in by 1:00 P.M. Monday thru Friday for United Parcel or Parcel Post shipments E-MAIL: [email protected] @westernranchsupply fax: 406-252-7282 To get the best out of every animal, we put the best into every animal. -

Horse Show Etiquette & Checklist
HORSE SHOW ETIQUETTE & CHECKLIST Good Etiquette for Horse Shows for Rider and Parent As a parent or supporter of a rider, you only want what's best for your child. After a great deal of practice and preparation, your rider is ready to show his or her skills in the competition arena. And there are things you can do to help. By following a few "etiquette" suggestions, you can make sure that your rider's horse show is an enjoyable and rewarding experience for everyone involved. During Show Preparations The coach or trainer's job is to help the rider perform her best. So, don't interfere when she/he is giving instructions before your child or rider goes into the show arena (unless it is absolutely 100 percent necessary, and if you do choose to do so, be sure to do it in a tactful way). You have hired a coach or trainer for a reason. Stand back and let him do his job. You'll be impressed. If the competition requires some sort of pattern or sequence of events, ask the rider to repeat the pattern back to you once. Have the pattern on a piece of paper handy in case the rider suddenly draws a blank. If this happens (not uncommon!), you will be a "super-parent or supporter of the show"! Do not drill the rider over and over again until you agitate them to the point that they lose their memory! Help the rider brush up right before entering the arena by checking for untucked shirts, loose hair-ties, crooked hats, uneven reins and the like. -

Flymask with Any Purchase of $100 Or More FREE Offer Applies for the First 2,000 Customers Only
Goodwoods Spring Specials Order 10%-50%off Online Airflow Summer Combo Now$ .95 only 49WAS $98.95 2 for $90.90 3 for $126.90 Flymask with any purchase of $100 or more FREE Offer applies for the first 2,000 customers only Airstream Mesh Combo Now$ .95 only 29WAS $59.95 2 for $55.90 3 for $75.90 Rainshield Unlined $ .95 Canvas Combo Now only 59WAS $80 2 for $110.90 3 for $155.90 Made of light-weight ripstop canvas, waterproof, Satin lined neck & shoulder Sizes 4’9” to 7’ Deluxe Tubular Lead Super Stick Elasticwrap Bandages Stock Saddle Carry Bag Assorted colours Available in Blue, Fluro Pink, Fluro Green, 2 Styles available: Stock, Western Fluro Purple. Mixed colours in a box available. & Swinging Fender. Made from 800 denier ripstop fabric Will fit the biggest stock saddles $ $ $ 9.95 3.00 BOX 49.95 EACH EACH OF 12$30 WAS $99.95 Flower Hackamore Felt Wither Pad Jump Boot Set Pony Mint, Lilac, Pink PVC Nose Black Shaped felt pad with breather holes to & Azure Blue aid circulation. Ideal for use as a front build-up pad. Tapered shape. Size: 57cm long x 52cm wide Brown. $ $ 79.00 $ 39.95 WAS $99.00 49.95 Economy Farrier Kit Tendon Boot Regal Pro III Compositi 2 Bar Stirrup Complete with Carry Roll Brown, Black & White Red, Royal, Light Also available in Blue, Pink & fetlock Black. small & large 2 $99.95 $64.95 $34.95 Crossover Ripstop $ .95 Mesh Combo Now only 59WAS $90 2 for $110.90 3 for $155.90 Made of light-weight ripstop fabric, Satin lined neck & shoulder Now with colours: white/white. -

Saddlery Inspections
Saddlery Inspections Rules and Procedures for Ring Stewards to conduct Saddlery Inspections in Dressage classes at USEF/USDF competitions April 2020 1 Saddlery Inspections Competition management must appoint a sufficient number of ring stewards to carry out the following duties: Communicate with the warmup steward and announcer, so that competitors can be kept informed as to who is “on deck” and whether the ring is running on time. Check saddlery and equipment, and the horse, after the specified number of rides. Inform judges of any delays or other concerns. Radio for help for ring repairs or emergencies, as directed according to the Accident Preparedness Plan. Depending on the layout, number of rings and other factors, more than one ring steward may be appointed to share these duties. 2 Saddlery Inspections Ring stewards must check saddlery and inspect bits and spurs on both sides of the horse for at least one- third of the horses in each class. In some classes, inspection is required for each horse. Inspection of saddlery and bits should be done at the direction of the Technical Delegate. 3 Saddlery Inspections Management must provide (preferably latex free) disposable protective gloves, at least two per horse. (Two gloves are required, one on each hand, for both USEF and FEI competitions.) The rider should see the inspector put on fresh gloves when the horse is exiting the arena. Inspection is done immediately after the performance ride. At no time should the horse, spurs or other equipment be touched with an “ungloved” hand, as the glove provides protection against the spread of disease. -

HORSE EXPO STUDY GUIDE Madera County 4-H Horse Level I & II HORSE EXPO STUDY GUIDE Madera County 4-H Level I & II
HORSE EXPO STUDY GUIDE Madera County 4-H Horse Level I & II HORSE EXPO STUDY GUIDE Madera County 4-H Level I & II Written Test Level I Level II Entry Form 22 28 Quiz Matching 15 15 Quiz Multiple Choice 15 10 Quiz True/False 5 Parts 20 33 Western Saddle 10 18 English Saddle 5 10 Bridles - English & Western 6/5 Sub-Total for Written Test 103 114 Expo Day Skills Level I Level II Feed ID 5 10 Equipment ID 15 20 Pre-Riding Skills 60 Vet Skills 60 Riding Skills 40 Showmanship Skills 25 30 Judging 10/10 10/10 Sub-Total for Skills Portion 125 180 Sub-Total for Written Test 103 114 Total for Expo Skills 228 294 Total Needed to Pass Level 182.4 235.2 Madera County Horse Expo 8/06 -1- PLEASE PRINT OR TYPE LEVEL I & II ___________________________________________________ HORSE ENTRY FORM ______ __________ ______ LAST NAME FIRST NAME MIDDLE INITIAL JUNIOR DEPARTMENT GRADE BIRTH DATE AGE ___________________________________________________ ALL DIVISIONS ADDRESS MADERA DISTRICT FAIR ________________________________________ ___________________________________________________ 25826 AVE. 15 ½ SIGNATURE OF LEGAL PARENT OR GUARDIAN CITY ZIPCODE PHONE MADERA, CA 93639 ___________________________________________________ 674-8511 SIGNATURE OF OWNER OR AGENT DATE _____________________________ DIVISION CLASS # CLASS DESCRIPTION NAME OF HORSE ENTRY FEE TOTAL FEE 1 2 3 4 5 6 7 8 9 10 CONSULT PREMIUM BOOK FOR DIVISION AND CLASS NUMBERS, ENTRY FEES, AND ENTRY CLOSING DATES TOTAL ENTRY FEES _____________________________ The undersign state herewith, that her/she is a recognized supervisor of the project of which the above entries are a part; that to his/her personal and actual knowledge the statements regarding the same are true; and he/she Amount Enclosed _____________________________ as read and has full understanding of the rules and regulations governing the Same and agrees to be governed by them. -
Steeplechase
Complimentary The Steeplechase A Publication of Vol. 17, No. 8 ST Publishing, Inc. Times Friday, September 24, 2010 Laughing all the way Lead Us Not helps Sheppard Stable rule Spa Inside This Edition Saratoga Racing Reports • Fall Preview Colonial Downs Coverage • Pick Six Update 2 • Steeplechase Times www.st-publishing.com • [email protected] Friday, September 24, 2010 News & Notes from around the circuit Tod Marks Summer Reading. ST went to Saratoga for the summer – where readers included Eclipse Award-winning jockey Garrett Gomez. “The farm life helps, you can keep them at a high-level of fitness but not By The Numbers have them mentally burnt out.” 27 Individual horses that started in the five steeplechase races at Sara- Danielle Hodsdon on the difference toga this summer. between training on the farm and at the track “You didn’t think Tom Voss was going to let that happen, did you?” 998 Career North American steeplechase victories (through Sept. 24) Trainer Todd Wyatt, after Voss won the Saratoga steeplechase for trainer Jonathan Sheppard. finale with Easy Red to deny Jonathan Sheppard a sweep Worth Repeating “If we won another jump race, they were going to replace Sea Hero with a “Most of our horses are homebreds on a very modest program. We’ve statue of Bill Pape – so it’s a good thing we got beat in that last one.” been lucky, we’ve been so many places with them. Nobody would have ever Sheppard, on the paddock statue (Sea Hero is safe) at Saratoga known me if I didn’t have Flatterer.” Owner Bill Pape, after winning the first four jump races at Saratoga “All of a sudden, we looked and we had eight horses and 18 stalls, we started picking up the phone and they started coming, just to fill the stalls.