Prevalence of Endodontic Diseases: an Epidemiological Evaluation in a Brazilian Subpopulation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
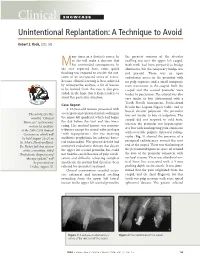
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

College Name: Dentistry University of Palestine Midterm Exam 1
Course No: DNTS3213 University of Palestine Instructor Name: Dr.Hadil Course Title: Endodontics Altilbani Date: 17 /11/2014 Student No.: _________________ No. of Questions: Midterm Exam Student Name: _______________ Time: 1hours 1st Semester 2014/2015 College Name: Dentistry SELECT THE MOST APPROPRIATE ANSWER: 1. Endodontic therapy is CONTRAINDICATED in teeth with 1. inadequate periodontal support. 2. pulp stones. 3. constricted root canals. 4. accessory canals. 5. curved roots. 2. A protective mechanism of the dental pulp to external irritation or caries is the formation of 1. pulp stones. 2. secondary dentin. 3. secondary cementum. 4. primary dentin. 3. If the maxillary first molar is found to have 4 canals, the 4th canal is most found: 1. In the disto-buccal root 2. In the mesio-buccal root 3. In the palatal root 4. All of the above 4. The " Working Length" of a tooth refers to: 1. The total length of a tooth from crown tip to root tip. 2. The measured length of a radiograph of the tooth. 3. The distance between a reference point on the crown and the apical limit of the tooth. 4. None of the above. [ 5. A central incisor diagnostic (pre operative) radiograph image measures 25mm from the incisal edge to the root apex. The estimated (initial) working length is : 1. 21mm 2. 25mm 3. 23mm 4. 27mm 6. Purpose of the access cavity 1. Access to the end of the root 2. Controlled instrument placement 3. Allow removal of debris 4. Allow introduction of materials and instruments 5. All of the above 1 Course No: DNTS3213 University of Palestine Instructor Name: Dr.Hadil Course Title: Endodontics Altilbani Date: 17 /11/2014 Student No.: _________________ No. -

Postgraduate Program in Endodontics
UNIVERSITY OF OSLO DENTAL FACULTY Department of Endodontics Postgraduate program in Endodontics Case book Birte Nikolaisen Myrvang Spring Semester 2006 Contents Case 1 Vital pulp therapy p. 3 Case 2 Vital pulp therapy of tooth with atypical canal morphology p. 9 Case 3 Chronic apical periodontitis p. 14 Case 4 Chronic apical periodontitis of tooth with dens invaginatus p. 20 Case 5 Chronic apical periodontitis of tooth with internal resorption p. 29 Case 6 Apical periodontitis with sinus tract p. 34 Case 7 Chronic apical periodontitis with exacerbation p. 39 Case 8 One-step treatment of chronic apical periodontitis p. 45 Case 9 Treatment of tooth with endodontic-periodontal involvement p. 49 Case 10 Retreatment of chronic apical periodontitis with a fractured instrument p. 55 Case 11 Chronic interradicular periodontitis with perforation p. 60 Case 12 Chronic apical periodontitis with multiple perforations p. 68 Case 13 Retreatment of a tooth with anatomically related sclerotic area p. 78 Case 14 Retreatment of a tooth with cervical resorption p. 83 Case 15 Radisectomy of an endodontic-periodontically involved tooth p. 91 Case 16 Retreatment of inadequately rootfilled tooth (24) and tooth with chronic apical periodontitis with a post (25) and vital pulp therapy (26) as a sequel to surgery. p. 96 Case 17 Surgical intervention of chronic apical periodontitis without retreatment p. 107 Case 18 Treatment of traumatically injured teeth in adult patient. p. 113 Case 19 Root canal treatment and surgery of medically compromised patient p. 120 Case 20 Pain management p. 129 2 Case 1 Vital pulp-therapy Symptomatic pulpitis of tooth 36 and 37 Patient A 28 year old caucasian female (figure 1) was referred from her general dental practitioner (GDP) to the Postgraduate Endodontic Clinic June 2003 for recurring pain from her left lower quadrant. -
An Introduction to Endodontics
FEATURE CPD: ONE HOUR An introduction to endodontics Images Plus ©wildpixel/iStock/Getty Peter V. Carrotte1 introduces the basic principles of endodontics and explains the difference between endodontics and root canal treatment. Introduction What is the difference between root canal treatment For many patients the thought of having to have a ‘root canal’ and endodontic treatment? causes fear and dread. All members of the dental team need to be Although the two terms are ofen used as if they mean the same, fully informed of exactly what this involves in order to put their root canal treatment is in fact just one part of endodontic treatment. minds at ease. Obviously the dentist will already be quite familiar Whenever any restorative dental treatment is carried out the dentist with these procedures, and the dental nurse will have a fairly has to protect the pulp from damage. Te total care of the pulp is good understanding. However, other members of the dental called endodontics. For example, if decay has spread very deeply team may not be quite so sure. into the tooth but the infection has not yet entered the pulp, the Here is an explanation of the processes involved so that dentist will seal the dentine tubules and may place a small amount of all members of the team can familiarise themselves with the calcium hydroxide on an exposed part of the pulp to promote normal procedures and the terminology associated with them. healing and keep the pulp alive. Tis would be endodontic treatment, but not root canal treatment. What is root canal treatment? Root canal treatment is carried out when the tooth’s pulp, Why would a patient need root canal treatment? the soft tissue core of the tooth containing the blood Root canal treatment is usually prescribed to relieve pain and there supply, nerves and connective tissue necessary for the are three classic painful conditions that may be diagnosed. -

Evaluation of Pathological Microbes in Root Canals with Pulp Necrosis
ORIGINAL RESEARCH Evaluation of Pathological Microbes in Root Canals with Pulp Necrosis Atul Anand Bajoria1, Ahmed Ali Alfawzan2, Vardharajula Venkata Ramaiah3, Mohammed Ali Habibullah4, Sabahat Ullah Tareen5, Prashant Babaji6 ABSTRACT Aim: The present study was conducted to evaluate the type of bacteria present in necrotic root canals of permanent teeth. Materials and methods: All 60 participants with infected root canals were made to use 10 mL of mouthwash containing 0.12% chlorhexidine. Access to pulp chamber was established, and the sterile absorbent paper cones were inserted into the canal for 20 seconds. The contaminated paper cones were inoculated in a brain–heart infusion (BHI) agar culture medium and incubated in an oven for 48 hours at 37°C. Results were analyzed statistically with SPSS version 20.0 using Chi-square test and analysis of variance (ANOVA). Results: In root canals with periapical lesions, gram-positive bacilli was present in 50 cases, gram-negative in 48 and yeast cells in 28; while in root canals without periapical lesions, gram-positive bacilli was present in 8. In 16 root canals of chronic apical periodontitis cases, gram-positive bacteria was present in 100%, gram-negative bacteria in 100%, and yeast cells in 20% cases. In 12 cases of periapical granuloma, gram-positive bacteria was present in 98%, gram-negative bacteria in 100%, and yeast cells in 40% cases. In 10 cases of chronic abscess with fistula, gram- positive bacteria was present in 86.2. In six cases of phoenix abscess, gram-positive bacteria was present in 100% and gram-negative bacteria in 100% cases. -

Management of Acute Periapical Lesions at Four Mandibular Incisors a Case Report
Case Report Adv Dent & Oral Health Volume 5 Issue 1 − June 2017 Copyright © All rights are reserved by Nedim Smajkic DOI: 10.19080/ADOH.2017.05.555654 Management of Acute Periapical Lesions at Four Mandibular Incisors a Case Report Nedim Smajkic* Specialist Endodontic, Private Dental Practice, Bosnia and Herzegovina Submission: May 07, 2017; Published: June 13, 2017 *Corresponding author: Nedim Smajkic DDS, MSc PhD, Private Dental Practice, St. Antuna Branka Simica 27, 71000 Sarajevo; Bosnia and Herzegovina, Tel: ; Email: Abstract extensive tissue destruction. This case report is showing the failures of previous endodontic treatment and apical surgery that resulted withDepending exacerbation on withthe severityphoenix ofabscess irritation, and tryduration, to preserve and host the fourresponse, teeth withperiradicular joined periapical pathology lesions may rangewith endodontic from mild retreatmentinflammation and to medicament therapy only. incisors were painful with swelling of soft tissue. After the emergency treatment, and endodontic therapy of all involved teeth during the periodFourteen of 10 months year old on female x-ray radiogrampatient addressed was noticed to the a dentallarge reduction office with of swelling radiolucency and pain in the in apicalthe mental region. area In ofthis the case, mandible. the used All medicament mandibular in combination with NiTi rotary instruments for root canal preparation and Gutta Flow with a gutta-percha point as obturation reduced the ofcause bone of defects. the acute periapical inflammation. -

DIAGNOSIS of PULPAL DISEASES Presenter: Dr. R.O. Kekere-Ekun Keywords: Diseases, Pulp, Diagnosis. OBJECTIVE Describe The
DIAGNOSIS OF PULPAL DISEASES Presenter: Dr. R.O. Kekere-ekun Keywords: Diseases, Pulp, Diagnosis. OBJECTIVE ● Describe the pulp, its functions and response to irritants/injuries. ● List the clinical classification of the diseases of the pulp. ● List the various causative factors involved in pulp diseases. ● Describe the diseases of the pulp in terms of signs and symptoms. ● Identify the potential sequelae of the diseases of the pulp. ● Itemize the essentials of diagnosis of the diseases of the pulp. ● List the various clinical examinations and tests that can be used to make a diagnosis for the diseases of the pulp as well as describe what the results of each test indicate. ● Describe how to conduct pulp tests and identify materials that can be used to conduct pulp tests. ● Describe the different clinical pulpal conditions according to the following aspects: –Patient dental history; –Patient signs and symptoms; –Pulp test results; –Radiographic findings. ● Note the top differential diagnosis of the diseases of the pulp. INTRODUCTION The dental pulp is a unique tissue and its importance in the long-term prognosis of the tooth is often ignored by clinicians. It is unique in that it resides in a rigid chamber which provides strong mechanical support and protection from the microbial rich oral environment. If this rigid shell loses its structural integrity, the pulp is under the threat of the adverse stimuli from the mouth, such as 1 caries, cracks, fractures and open restoration margins, all of which provide pathways for micro-organisms and their toxins to enter the pulp. The pulp initially responds to irritation by becoming inflamed and, if left untreated, this will progress to pulp necrosis and infection. -
Identify and Define All Diagnostic Terms for Periapical/Periradicular
Review Article Identify and Define All Diagnostic Terms for Periapical/ Periradicular Health and Disease States James L. Gutmann, DDS,* J. Craig Baumgartner, DDS, MS, PhD,† Alan H. Gluskin, DDS,‡ § Gary R. Hartwell, DDS, MS, and Richard E. Walton, DMD, MSjj Abstract Introduction: The purpose of this in-depth investigation ne of the hallmarks of any profession is its distinct lexicon; this is no different with was to identify, clarify, and substantiate clinical terminology Othe dental specialties. Within this framework of the lexicon, there should exist relative to apical/periapical/periradicular diagnostic states, clarity, succinctness, and specificity that are based on sound biological principles which is used routinely in the provision of endodontic and understandings, clinical realities, and daily usages. Even in a global society in which care. Furthermore, the information gleaned from this inves- differences may exist, there must be a commonality of thought, a distinct explicitness of tigation was used to link diagnostic categories to symp- meaning, and a rational basis for the choice of terminology and its routine application, toms, pathogenesis, treatment, and prognosis wherever as opposed to personalized, empiric bias that is used to exaggerate an individual’s possible, along with establishing the basis for the metrics thought process or perceived and unsupported interpretation. Oftentimes, the latter used in this diagnostic process. Materials and Methods: is identified as colloquial and bears little resemblance to the actual issue, event, or Diagnostic terminologies and their relevance to clinical procedure at hand. Within the discipline of endodontics, this latter type of lexicon situations were procured from extensive historic and elec- has been proffered in contemporary times regardless of the historic framework on tronic searches and correlatedwithcontemporaryconcepts which it has evolved. -
Apical Periodontitis: Etiology, Pathogenesis, Classification
APICAL PERIODONTITIS: ETIOLOGY, PATHOGENESIS, CLASSIFICATION Minsk BSMU 2016 МИНИСТЕРСТВО ЗДРАВООХРАНЕНИЯ РЕСПУБЛИКИ БЕЛАРУСЬ БЕЛОРУССКИЙ ГОСУДАРСТВЕННЫЙ МЕДИЦИНСКИЙ УНИВЕРСИТЕТ 1-я КАФЕДРА ТЕРАПЕВТИЧЕСКОЙ СТОМАТОЛОГИИ АПИКАЛЬНЫЙ ПЕРИОДОНТИТ: ЭТИОЛОГИЯ, ПАТОГЕНЕЗ, КЛАССИФИКАЦИЯ APICAL PERIODONTITIS: ETIOLOGY, PATHOGENESIS, CLASSIFICATION Рекомендовано Учебно-методическим объединением по высшему медицинскому, фармацевтическому образованию Республики Беларусь в качестве учебно-методического пособия для студентов учреждений высшего образования, обучающихся на английском языке по специальности 1-79 01 07 «Стоматология» 2-е издание Минск БГМУ 2016 2 УДК 616.314.17-008.1-02-092(811.111)-054.6(075.8) ББК 56.6.(81.2 Англ-923) А76 А в т о р ы: Л. А. Казеко, Ю. В. Модринская, К. В. Севрукевич, E. Л. Колб Р е ц е н з е н т ы: д-р мед. наук, проф., зав. каф. общей стоматологии Белорусской медицинской академии последипломного образования Н. А. Юдина; каф. терапевтичес- кой стоматологии Витебского государственного ордена Дружбы народов медицинского университета Апикальный периодонтит : этиология, патогенез, классификация = Apical perio- А76 dontitis : etiology, pathogenesis, classification : учеб.-метод. пособие / Л. А. Казеко [и др.]. – 2-е изд. – Минск : БГМУ, 2016. – 16 с. ISBN 978-985-567-453-6. Рассматриваются вопросы этиологии, патогенеза и классификации апикального периодонтита. Материал базируется на имеющихся в отечественной и зарубежной литературе современных представлениях по данной проблеме. Первое издание вышло в 2015 году. Предназначено для студентов 3-го курса медицинского факультета иностранных учащихся, обучающихся на английском языке. УДК 616.314.17-008.1-02-092(811.111)-054.6(075.8) ББК 56.6.(81.2 Англ-923) ISBN 978-985-567-453-6 © УО «Белорусский государственный медицинский университет», 2016 3 DEFINITION The periodontium comprises the root cementum, the periodontal ligament and the alveolar bone. -

Review Article
z Available online at http://www.journalcra.com INTERNATIONAL JOURNAL OF CURRENT RESEARCH International Journal of Current Research Vol. 8, Issue, 11, pp.42447-42450, November, 2016 ISSN: 0975-833X REVIEW ARTICLE CLINICAL DIAGNOSIS OF DENTAL PAIN *Dr. Aji Markose Department of Conservative Dentistry, Vivekanada Dental College, Thiruchengode (Namakkal dt), Tamilnadu - 637205 ARTICLE INFO ABSTRACT Article History: Dental pulp consist of vascular connective tissue contained within the rigid dentin walls. It is the th principal source of pain in the oral cavity and also a major site of attention in endodontics and Received 08 August, 2016 Received in revised form restorative procedures. Thus the knowledge to pulp is essential not only for providing dental treatment 25th September, 2016 but also to know the rationale behind the treatment provided. Accepted 19th October, 2016 Published online 30th November, 2016 Key words: Dental pulp, Pain, Inflammation, Pulpitis, Dentin, Tooth fracture. Copyright©2016, Aji Markose. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Citation: Aji Markose, 2016. “Clinical diagnosis of dental pain”, International Journal of Current Research, 8, (11), 42447-42450. INTRODUCTION Radiographs: The dental pulp is subjected to various insults in the Show normal PDL and lamina dura mouth.These may be in the form of physical, chemical or Depth of caries or restoration may be evident bacterial agents.The pulp responds to these irritants most often by an inflammatory response and sometimes by pulpal Percussion test: Shows negative response i.e tooth is normal degeneration.The nature of the irritant and the duration of to percussion and palpation without any mobility. -

ADA.Org: NBDE Part II Endontics Terminology
IMPORTANT NOTE CONCERNING NBDE PART II ENDODONTICS TERMINOLOGY Although the new endodontic terms adopted by the American Association of Endodontists were anticipated to be incorporated into the NBDE Part II in 2012, technical issues were encountered that caused an unexpected delay. These terms will now be implemented in 2013. During this transitionary period, it is recommended that individuals become knowledgeable of both sets of terms, because individual researchers, practitioners, and existing textbooks can communicate information using either set of terms. The NBDE Part II Guide has been updated to reflect this change. 12/5/12 UPDATE: Based on feedback from test constructors, the American Association of Endodontists has provided the Joint Commission with an updated chart to assist students who are currently taking NBDE Part II: OLD TERM NEW TERM DEFINITION Normal Pulp Normal Pulp A clinical diagnostic category in which the pulp is symptom-free and normally responsive to pulp testing. Reversible Pulpitis Reversible Pulpitis A clinical diagnosis based upon subjective and objective findings indicating that the inflammation should resolve and the pulp return to normal. Irreversible Pulpitis Symptomatic A clinical diagnosis based on subjective and objective findings Irreversible Pulpitis indicating that the vital inflamed pulp is incapable of healing. Additional descriptors: Lingering thermal pain, spontaneous pain, referred pain. *Irreversible Pulpitis Asymptomatic A clinical diagnosis based on subjective and objective findings Irreversible Pulpitis indicating that the vital inflamed pulp is incapable of healing. Additional descriptors: No clinical symptoms but inflammation produced by caries, caries excavation, trauma, etc. Pulp Necrosis Pulp Necrosis A clinical diagnostic category indicating death of the dental pulp. -

SNODENT (Systemized Nomenclature of Dentistry)
ANSI/ADA Standard No. 2000.2 Approved by ANSI: December 3, 2018 American National Standard/ American Dental Association Standard No. 2000.2 (2018 Revision) SNODENT (Systemized Nomenclature of Dentistry) 2018 Copyright © 2018 American Dental Association. All rights reserved. Any form of reproduction is strictly prohibited without prior written permission. ADA Standard No. 2000.2 - 2018 AMERICAN NATIONAL STANDARD/AMERICAN DENTAL ASSOCIATION STANDARD NO. 2000.2 FOR SNODENT (SYSTEMIZED NOMENCLATURE OF DENTISTRY) FOREWORD (This Foreword does not form a part of ANSI/ADA Standard No. 2000.2 for SNODENT (Systemized Nomenclature of Dentistry). The ADA SNODENT Canvass Committee has approved ANSI/ADA Standard No. 2000.2 for SNODENT (Systemized Nomenclature of Dentistry). The Committee has representation from all interests in the United States in the development of a standardized clinical terminology for dentistry. The Committee has adopted the standard, showing professional recognition of its usefulness in dentistry, and has forwarded it to the American National Standards Institute with a recommendation that it be approved as an American National Standard. The American National Standards Institute granted approval of ADA Standard No. 2000.2 as an American National Standard on December 3, 2018. A standard electronic health record (EHR) and interoperable national health information infrastructure require the use of uniform health information standards, including a common clinical language. Data must be collected and maintained in a standardized format, using uniform definitions, in order to link data within an EHR system or share health information among systems. The lack of standards has been a key barrier to electronic connectivity in healthcare. Together, standard clinical terminologies and classifications represent a common medical language, allowing clinical data to be effectively utilized and shared among EHR systems.