Report on Additional Work Completed Following Designation Workshop (29 June 2005)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Clinical System Framework Launch
Care to Share Issue 11 Spring 2021 Clinical System Framework Launch Our shared vision for continuous improvement, providing safe, effective and high quality care for all our service users. Reflections on my Nursing Reaping the Rewards British Journal of AHP Career Associates of Research Nursing Award Winner Page 4 Page 6 Page 17 Page 20 Contents P5 Issue 11 / Spring 2021 Page Welcome to RWT – Katrina Creedon and Ruth Spedding 3 Ravi Goyal and Carol Morris, Volunteers Reflections on my AHP Career 4 Community Clinical Volunteer Programme 5 P11 Nursing Associates 6 Urology Cancer Care Navigator 7 Serious Case Reviews 8-9 Donation by Orthotics Team 9 Emotional Wellbeing Support 10 Lisa Lawton, Matron for Pre-Registrant Nurse Education Welcome to RWT – Lisa Lawton 11 Meridian Celebration of Innovation Awards 11 P12-15 The Clinical System Framework 12-15 Competency Project 16 Reaping the Rewards of Research 17 The RWT Dignity Awards 2020 17 News in Brief 18-19 British Journal of Nursing Award Winner 20 A message from Professor Ann-Marie Cannaby Dear colleagues, will be mainly focussed on the new CSF the COVID-19 crisis. We can use the CSF along with the usual news, views and best to refocus, reframe what we are doing This Spring Edition of ‘Care to Share’ practice announcements to share with and look ahead. I continue to thank sees the beginning of longer and lighter you. you all and ask you to be proud of your days for us all and the signs of new life achievements. in the trees, hedgerows and the much The CSF is a two year detailed strategy of welcomed arrival of the seasonal plants how we as nurses, midwives and health Stay safe, such as daffodils and crocuses. -

Primary Biliary Cirrhosis
Gut: first published as 10.1136/gut.24.10.940 on 1 October 1983. Downloaded from Gut, 1983, 24, 940-945 Liver and biliary Primary biliary cirrhosis: geographical clustering and symptomatic onset seasonality A N HAMLYN, A F MACKLON, AND 0 JAMES From the University Departments of Medicine and Geriatrics, Freeman Hospital, Newcastle-upon-Tyne SUMMARY Patients with primary biliary cirrhosis (primary non-suppurative destructive cholangitis) in the north east region of England were studied over a five year period and, to evaluate epidemicity, compared with two contemporaneous disease series of known occurrence. These were: terminal renal failure, all causes (low or absent epidemicity n= 106) and an outbreak of echovirus 19 disease (high epidemicity n=201). Eight primary biliary cirrhosis-affected men and 109 women from an estimated catchment population of 2.08 million were identified. The current diagnosis rate was 1.0/100 000 (1-8/100 000 for women of 15 or more). There were 18 deaths, mean survival from diagnosis 4.0 years. Within the region prevalence varied from 3.7/100 000 in rural areas to 14-4/100 000 in industrial urban areas. In the conurbation, prevalence rates varied insignificantly. Here, most cases were concentrated in central districts, where the proportion of asymptomatic presentations was 50%. Outside the conurbation the asymptomatic proportion fell to 21%, suggesting low incidental diagnosis rates. When compared with echovirus 19, primary biliary cirrhosis was of low or absent epidemicity, and similar to renal failure in its uniform geographical distribution and lack of clustering. Forty three patients (37% of the total), however, had significantly seasonal symptomatic presentations (p<0.01), although scan statistic testing failed to show clustering of onset in time. -
Planning Application Number:P15/1394
PLANNING APPLICATION NUMBER:P15/1394 Type of approval sought Outline Planning Permission Ward Wordsley Applicant NHS Property Services Location: RIDGE HILL, BRIERLEY HILL ROAD, WORDSLEY, STOURBRIDGE, DY8 5ST Proposal OUTLINE PLANNING PERMISSION WITH ALL MATTERS RESERVED APART FROM ACCESS, TO ALLOW THE DEVELOPMENT OF UP TO 129 RESIDENTIAL DWELLINGS FOLLOWING THE DEMOLITION OF THE KEELING CENTRE AND SHOUSTERS HOUSE. Recommendation APPROVE SUBJECT TO CONDITIONS AND 106 Summary: SITE AND SURROUNDINGS 1. The site measures a total of 4.16 hectares and comprises the former Ridge Hill hospital site accessed off Brierley Hill Road. The majority of the buildings have been demolished with the exception of the former nursing home located within the south- west of the site and two single storey buildings within the northern part of the site (Shousters House and the Keeling Centre). The retained buildings are vacant and unused. 2. The site is accessed from Brierley Hill Road. The main access road into the site off Brierley Hill Road adjoins an access that serves The Wordsley School. The estate road into the hospital complex does not comprise any pedestrian or cycle footways. The estate road into the site crosses over a culverted watercourse. The access into the site from Brierley Hill Road adjoins a signalised crossing of which part of the controlled area of the crossing falls within the existing access road into the site. 3. The site adjoins a number of existing uses that would be retained as a result of the development including The Ridge Hill Centre LIFT building and associated residential care units (Meadows Rise and Brooks Mead), Pens Meadow School, a 1 special school for children and young adults and a small development of bungalows providing assisted living within the north-western part of the site. -

Holy Trinity Church Amblecote - Burial Register from 8Th December, 1996
HOLY TRINITY CHURCH AMBLECOTE - BURIAL REGISTER FROM 8TH DECEMBER, 1996 Entry Name Address Date of death Age Date of Burial Plot ref 1997 801 FLORIDA Cyril William John 2, Grampian Road 08.12.1996 77 16.12.1996 O48 802 PITT Dora Valenteen Comberton Nursing Home 19.01.1997 92 30.01.1997 D111 803 BOWES Dorothy Anne 38, High Street 05.02.1997 77 14.02.1997 O47 804 FISHER Hilda Mary 91, Trinity Road 15.03.1997 85 24.03.1997 O46 805 HAYES Joseph William Daniel Lodge Home, 69a Vicarage Rd 28.03.1997 83 12.04.1997 P52 806 JONES Gladys Maud (Crem. Remains) Formally 22, School Drive 05.04.1997 93 17.04.1997 B164 807 CARTWRIGHT Alice Elizabeth (C. R.) 24.03.1997 72 21.04.1997 B135 808 DOVEY Ralph Norman 46, Platts Crescent 15.04.1997 64 21.04.1997 P51 809 HAZELDINE William Herbert 2, Whitethorne Road, Wordsley 02.06.1997 77 06.06.1997 P50 810 JEAVONS Kenneth Albert (C. R.) 111, King William Street 24.09.1997 72 09.10.1997 F14 811 BROOKS Eileen Maud 1, Stawton House, Christchurch St, Cambridge 22.10.1997 86 31.10.1997 P49 812 MOBBERLEY Alan Edwin Wellings Cottage, Morfe Lane, Enville 19.10.1997 70 01.11.1997 A12 813 PRICE Michael Neil (Crem. Remains) 11, Milton Close 08.10.1997 59 03.11.1997 G1 814 GHALI Anis Aziz 42, Lynwood Avenue, Wall Heath 13.11.1997 58 21.11.1997 P48 815 CARTWRIGHT Florence Amblecote House, King William Street 27.11.1997 83 05.12.1997 P47 816 DRUCE John Franklin (Crem. -

West Midlands
Archaeological Investigations Project 2005 Building Survey West Midlands Birmingham Area Birmingham (G.06.4153) SP05768650 {C0E77FCB-9C21-4D4E-BDBC-9464D68DC566} Parish: Birmingham Postal Code: B16 8HW NEW UNION MILL New Union Mill, Grosvenor Street West, Birmingham Hislop, M Birmingham : Birmingham Archaeology, 2005, 15pp, colour pls, figs, tabs, refs Work undertaken by: Birmingham Archaeology Archaeological periods represented: PM (G.06.4154) SP14209680 {E859A766-AC7F-40D0-AA12-9213CEA9DDCC} Parish: Sutton Coldfield Postal Code: B75 6JD BARN FARM, SUTTON COLDFIELD Barn Farm, Lindridge Road, Sutton Coldfield, Birmingham Lowe, J Cheltenham : CgMs, 2005, 165pp, colour pls, figs, tabs, refs Work undertaken by: CgMs Archaeological periods represented: PM Coventry (G.06.4155) SP33457925 {CCB3E010-8794-4B31-86B1-F24E1D76D389} Parish: Coventry Postal Code: CV1 5PW THE FORMER LEA-FRANCIS WORKS The Building History of the Former Lea-Francis Works in Lower Ford Street, Coventry Litherland, S Birmingham : Birmingham Archaeology, 2005, 33pp, colour pls, figs, tabs, refs Work undertaken by: Birmingham Archaeology Archaeological periods represented: PM Dudley (G.06.4156) SO97308370 {218D1220-D47C-4510-B669-113A67368CC5} Parish: Halesowen Postal Code: B62 8DR 19 GREEN HILL ROAD, MUCKLOW HILL 19 Greenhill Road, Mucklow Hill, Halesowen Stansgate Straford-upon-Avon : Stansgate, 2005, 10pp, colour pls, figs, tabs, refs Work undertaken by: Stansgate Archaeological periods represented: PM (G.06.4157) SO94088640 {1F266B96-73EF-4D7D-BF35-AB1A22BD4FC6} Parish: -

Burial Register 1904 - 1921
HOLY TRINITY CHURCH AMBLECOTE - BURIAL REGISTER 1904 - 1921 Entry Name Address Date of death Age Date of Burial Plot ref 1904 1 GUNN Charles 16, Rosamund Street, Walsall 84 18.06.1904 2 MOODY Lydia Brettell Lane, Amblecote 75 19.06.1904 3 SMITH John Amblecote Infant 22.06.1904 4 SUTTON William 23, Coalborn Brook, Amblecote 63 25.96.1904 5 PITT Annie Lottie Amblecote Villa, Amblecote 28 28.06.1904 6 KEENE Isabel Winifred 5, Villa Street 1 29.06.1904 7 BRISTOW Rosanna 26, Box Hill, Amblecote 1 28.06.1904 8 JAMES Alice Maud Vale Street, Amblecote 1 30.06.1904 9 DOUGHTY Alfred Bell Kidderminster (Suicide Vicarage Road Bridge) 43 04.07.1904 10 MOLINEUX Henry 3, Vicarage Road 77 05.07.1904 11 VALE Harriet 28, Park Street, Brierley Hill 89 05.07.1904 12 TOLLEY Beatrice 6, Box Hill, Amblecote 3 07.07.1904 13 PEARSON Flora Ida 79, Worcester Street 63 11.07.1904 14 BYWATER John 2, Box Hill 2 12.07.1904 15 HILL William 98, King William Street 40 23.07.1904 16 ASHTON Ann Amblecote Road, Delph, Brierley Hill 64 27.07.1904 17 LOASBY Amelia Maria 15, High Street, Amblecote 63 03.08.1904 18 PLANT Job 77, Birmingham Street 44 14.08.1904 19 HILL Violet May 11, Withymoor, Amblecote Infant 22.08.1904 20 PRICE Cooksey 56, Moor Street, Brierley Hill 64 03.09.1904 21 HADEN John William 20, Box Hill Infant 03.09.1904 22 ZINKE Agnes Annie 13, Brettell Lane 55 03.09.1904 23 TURNER Mary 113, Enville Street 71 08.09.1904 24 HAMBREY Skidmore Platts Crescent 62 14.09.1904 25 DINGLEY John 67, Worcester Street 76 16.09.1904 26 ALLCHURCH Mary Ann 55, Collis Street 52 -
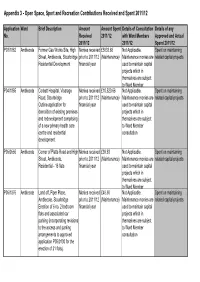
Appendix 3 - Open Space, Sport and Recreation Contributions Received and Spent 2011/12
Appendix 3 - Open Space, Sport and Recreation Contributions Received and Spent 2011/12 Application Ward Brief Description Amount Amount Spent Details of Consultation Details of any No. Received 2011/12 with Ward Members Approved and Actual 2011/12 2011/12 Spend 2011/12 P03/1862 Amblecote Former Gas Works Site, High Monies received £5833.68 Not Applicable. Spent on maintaining Street, Amblecote, Stourbridge prior to 2011/12 (Maintenance) Maintenance monies are related capital projects Residential Development financial year used to maintain capital projects which in themselves are subject to Ward Member P04/1865 Amblecote Corbett Hospital, Vicarage Monies received £10,520.66 Not Applicable. Spent on maintaining Road, Stourbridge prior to 2011/12 (Maintenance) Maintenance monies are related capital projects Outline application for financial year used to maintain capital demolition of existing premises projects which in and redevelopment comprising themselves are subject of a new primary health care to Ward Member centre and residential consultation development. P05/0556 Amblecote Corner of Platts Road and High Monies received £39.93 Not Applicable. Spent on maintaining Street, Amblecote, prior to 2011/12 (Maintenance) Maintenance monies are related capital projects Residential - 16 flats financial year used to maintain capital projects which in themselves are subject to Ward Member P05/1876 Amblecote Land off, Piper Place, Monies received £48.50 Not Applicable. Spent on maintaining Amblecote, Stourbridge prior to 2011/12 (Maintenance) Maintenance monies are related capital projects Erection of 6 no. 2 bedroom financial year used to maintain capital flats and associated car projects which in parking (incorporating revisions themselves are subject to the access and parking to Ward Member arrangements to approved consultation application P05/0130 for the erection of 21 flats). -

Holy Trinity Church Amblecote - Burial Register 1942 to 1954
HOLY TRINITY CHURCH AMBLECOTE - BURIAL REGISTER 1942 TO 1954 Entry Name Address Date of death Age Date of Burial Plot ref 1942 1 HEATHCOCK James 47, King William Street 78 04.03.1942 2 TREVIS Eliya 12, Delph Road, Brierley Hill 82 18.03.1942 3 WHITEHOUSE Thomas 23, King William Street 58 28.03.1942 4 CARTWRIGHT William Henry 123, High Street, Amblecote 62 28.03.1942 5 GRIFFITHS Clara 155, King William Street 73 30.03.1942 6 BROOKS Noah 4, Hill Street, Wollescote 72 09.04.1942 7 ALLPORT William District Hospital, West Bromwich 69 18.04.1942 8 COOPER Elizabeth 143, King William Street 72 25.04.1942 9 NEVENS Emily Bertha 29, Platts Crescent 63 16.05.1942 10 WINNALL Sarah Maria 4, Vicarage Road, Amblecote 74 08.06.1942 11 SAUNDERS Richard 44, Collis Street 72 19.06.1942 12 SCOTT Mary Ann 47, Platts Crescent 85 10.06.1942 13 POTTS Frederick John "Douston" Apley Road, Wollaston 55 08.07.1942 14 VENABLES Emily Gertrude Sandfield House, Wordsley (Brettell Lane) 74 28.07.1942 15 GARRATT Alice Emma 1a, Raddlebarn Road, Selly Oak, Birmingham 90 29.07.1942 16 JEFFRIES Sheila "St Davids", Barnett Lane, Wordsley 4 hrs 04.08.1942 17 JEFFRIES Michael Frederick "St Davids", Barnett Lane, Wordsley 4 hrs 04.08.1942 18 LAWRENCE George Humphrey 48, Corbett Crescent 50 27.08.1942 19 CARTWRIGHT Sarah Maria 30, Thorms Road, Quarry Bank 64 01.09.1942 20 BRYCE George 101, King William Street 63 10.09.1942 21 SMITH Elizabeth Corbett Hospital, Amblecote (off Platts Lane) 60 24.09.1942 22 DAVIESusan 207, Brettell Lane 76 03.10.1942 23 ALLPORT Mary 51, School Lane, Quarry Bank 72 08.10.1942 24 CARTWRIGHT William 10, Dunns Bank, Quarry Bank 76 02.11.1942 25 HANCOX Laura 118, King William Street 54 09.11.1942 26 WEBB Florence Rosa Newlands Nursing Home, Rabe, Liss R.D. -

Willetts Lodge, Clock Tower View, Wordsley, DY8 5TJ Offers Over
Willetts Lodge, Clock Tower View, Wordsley, DY8 5TJ WILLETTS LODGE WHICH FORMS PART OF THE 'HERITAGE BUILDINGS' | WELL PRESENTED SPACIOUS TOP FLOOR APARTMENT | OPEN PLAN LIVING ACCOMMODATION | FEATURE HIGH CEILINGS AND SASH WINDOWS MASTER BEDROOM WITH EN SUITE SHOWER ROOM | TWO DOUBLE BEDROOMS | ALLOCATED PARKING SPACE WITH FURTHER VISITOR SPACES | INVITING ENTRANCE HALLWAY Offers Over: £130,000 Willetts Lodge, Clock Tower View, Wordsley, DY8 5TJ This well presented two bedroom top floor apartment in Willetts Lodge which forms part of the Old Wordsley Hospital 'Heritage Buildings' comprises: communal hall, inviting entrance hallway, open plan living accommodation, master bedroom with en suite shower room, further double bedroom and a bathroom. This stunning apartment has feature high ceilings, sash windows and comes with an allocated parking space with further visitor spaces. FRONT OF THE PROPERTY Forming part of the 'Heritage Buildings' Willetts BEDROOM ONE Lodge is accessed via Kirkpatrick Drive, there is a 3.94m (12' 11") x 2.57m (8' 5") door to the rear of the Lodge which gives access to With a door leading from the entrance hall, double the communal hallway. glazed sash window to the side, door leading to the en suite and an electric heater. ENTRANCE HALL With access via the communal hallway and stairs, this inviting hall has doors to various rooms, telephone entry system, electric heater and a useful storage cupboard. EN SUITE With a door leading from the bedroom, shower cubicle, WC, wash hand basin, extractor fan and an electric heater. OPEN PLAN LIVING ACCOMMODATION 5.49m (18' 0") x 5.33m (17' 6") With a door leading from the hall this open plan living accommodation has a modern kitchen which is fitted with a range of wall and base units, work surfaces with matching splash back, stainless steel sink and drainer, integrated electric oven and electric hob with a stainless steel cooker hood over, plumbing for a washing machine and space for a fridge. -

Developing a Centralised Community Paediatric Centre for Dudley
4.2 Agenda Item -8 Health Select Committee Subject: Developing a Centralised Community Paediatric Centre for Dudley Presented by: Ann-Marie Morris, Strategic Lead – Children, Families and Young People Adrian Hulford, Deputy Director Community Services Aim of the report: To update the Health Select Committee on the strategic intent for development of a Community Paediatric Centre for Dudley; the establishment of a Steering Group to develop proposals and procure construction of the building; and to identify progress with interim proposals for clinical facilities and office base for the paediatric therapy services in preparation for sale of the Ridge Hill site for redevelopment. Key points: The strategic development of integrated services for children includes the development of a Centralised Community Paediatric Centre. Discussions have been ongoing on a multi-agency basis between hospital paediatric consultants, community services paediatric teams, GP representatives and Dudley MBC since 2004. A Steering Group is being established to drive forward the consolidation of proposals, consult on the range of services to be co-located, and oversee the design and construction procurement for the Centre. Given that the timescale for the development is out of synchronisation with the closure and sale of the current base for Paediatric Therapy Clinics at Ridge Hill Hospital, interim facilities are being refurbished to provide a fixed term clinical/office base whilst the Dudley Community Paediatric Centre is designed and built. Report is for Information Key Standard for Better Health: C5,C6, C7, C13, C17, C20, C21, D5, D8 Implications: Financial: The Steering Group will identify additional costs for construction/leasing of the Dudley Centralised Community Paediatric Centre. -

WEST MIDLANDS TRAMWAYS – SL 239 20.01.20 Page 1 of 7 FARE STAGES and Other Main Stops
1 WEST MIDLANDS TRAMWAYS – SL 239 20.01.20 page 1 of 7 FARE STAGES and other main stops See also General Notes at head of ENGLAND TRAMWAYS list. £ or no symbol: fare stage (FS) name in fare tables or on tickets; t: name in public timetables (TT)/destination screens + other /very likely main stops (e.g. at railway stations, town halls, selected loops (L). #: names from histories; u/d: undated Former names: [ ]; i.d: stop only in this direction; o.d: stop only in other direction; tm: terminus For system maps, The Tramways of the West Midlands issued by the Light Rail Transit Association is recommended BIRMINGHAM CORPORATION TRAMWAYS √ Warner Street 1930 /1946 fare tables, tickets, Stratford Place routes are grouped together with fare stages as 1930 Guide Farm Road “occasional services” (peak hours etc) not included Ladypool Road Stoney Lane-Stratford Road Junction / Walford Road Routes 1 & 78 Stoney Lane Terminus Steelhouse Lane General Hospital +(bus FS) Route 5 Gosta Green Soho Road (Villa Road) Dartmouth Street Hamstead Road-Villa Road Junction Phillips Street Burbury Street Aston Cross Berners Street Aston Station Wheeler Street-Lozells Road Junction Slade Road Junction, Lichfield Road Six Ways, Aston George Road Park Road, Aston Hunton Hill Aston Station Stockland Green £ Slade Road Junction, Lichfield Road Marsh Lane [Village Green £ ] Short Heath Road Terminus Route 6 Martineau Street (as 3 to:) Route 2 Six Ways, Aston Steelhouse Lane (as 1 to:) Fentham Road, Birchfields [Chain Walk here] Slade Road Junction, Lichfield Road Perry Barr Terminus Kingsbury Road Hunton Hill [Station Road, Gravelly Hill ] Route 7 cl. -

Burial Records 1954-1996
HOLY TRINITY CHURCH AMBLECOTE - BURIAL REGISTER October 1954 - December 1996 Entry Name Address Date of death Age Date of Burial Plot ref 1954 1 WALKER Major Thomas Wordsley Hospital (80, Collis Street) 68 27.10.1954 I43 2 DOVEY Beatrrice Wordsley Hospital 60 08.11.1954 I44 3 WILKES Walter Wildred 6, Collis Street 69 13.11.1954 I45 4 HORTON Elizabeth The Royal Oak, High Street 86 20.11.1954 E-Q9 5 BUDGE Arthur Samuel 25, Platts Crescent 72 01.12.1954 B-J7 6 DAVIES Clarence Edward 114, King William Street 60 18.12.1954 New 2-2 7 HARRIS Alice 10, 10, Burton Road, Sedgley 96 22.12.1954 B-N6 8 GRAHAM Thomas Whittle 71, Collis Street 61 29.12.1954 E-E1A 1955 9 WATSON Elsie 6, Giles Hill, Stourbridge 57 12.01.1955 D-I25 10 LOWE Fred 65, Brettell Lane 58 15.01.1955 C-A 11 HEATHCOCK John Lawrence 55, Delph Lane, Brierley Hill 87 10.02.1955 New 1-46 12 ASTON Thomas 100, Amblecote Road, Brierley Hill 78 21.02.1955 New 1-47 13 CHANCE Albert Edward Yardley Green Hospital (19, Brettell Lane) 41 23.02.1955 New 1-48 14 HILL Precilla 137, Brettell Lane 74 25.02.1955 B-M2 15 PRICE Mary Ann 122, King William Street 84 28.02.1955 B-M2 16 SHORT John Albert 190, Amblecote Road, Brierley Hill 68 01.03.1955 C-Row 3 17 SIMPSON Harriet 125, King William Street 85 01.03.1955 E-F35 18 HEATHCOCK Pheobe 3, Amblecote Road, Quarry Bank 84 04.03.1955 New 1-46 19 WOOLDRIDGE Vernon 51, Vicarage Road 62 12.03.1955 New 2-4 20 COMPSON Mary 36, Coventry Street, Stourbridge 82 22.03.1955 B-M24 21 WOODYATT Ellen 73, Platts Crescent 82 01.04.1955 New 2-5 22 WILKES Sarah Annie