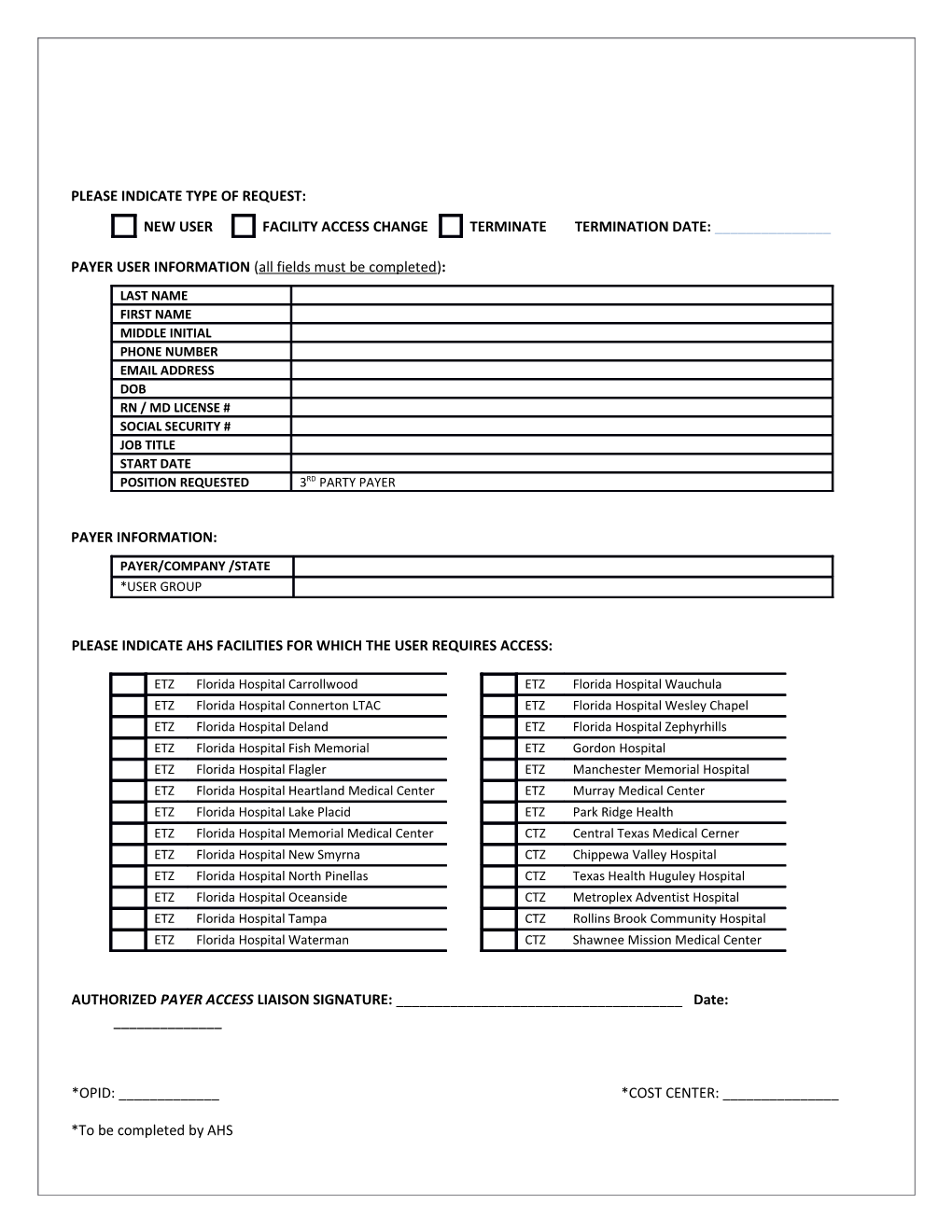
PLEASE INDICATE TYPE OF REQUEST: NEW USER FACILITY ACCESS CHANGE TERMINATE TERMINATION DATE: ______
PAYER USER INFORMATION (all fields must be completed): LAST NAME FIRST NAME MIDDLE INITIAL PHONE NUMBER EMAIL ADDRESS DOB RN / MD LICENSE # SOCIAL SECURITY # JOB TITLE START DATE POSITION REQUESTED 3RD PARTY PAYER
PAYER INFORMATION: PAYER/COMPANY /STATE *USER GROUP
PLEASE INDICATE AHS FACILITIES FOR WHICH THE USER REQUIRES ACCESS:
ETZ Florida Hospital Carrollwood ETZ Florida Hospital Wauchula ETZ Florida Hospital Connerton LTAC ETZ Florida Hospital Wesley Chapel ETZ Florida Hospital Deland ETZ Florida Hospital Zephyrhills ETZ Florida Hospital Fish Memorial ETZ Gordon Hospital ETZ Florida Hospital Flagler ETZ Manchester Memorial Hospital ETZ Florida Hospital Heartland Medical Center ETZ Murray Medical Center ETZ Florida Hospital Lake Placid ETZ Park Ridge Health ETZ Florida Hospital Memorial Medical Center CTZ Central Texas Medical Cerner ETZ Florida Hospital New Smyrna CTZ Chippewa Valley Hospital ETZ Florida Hospital North Pinellas CTZ Texas Health Huguley Hospital ETZ Florida Hospital Oceanside CTZ Metroplex Adventist Hospital ETZ Florida Hospital Tampa CTZ Rollins Brook Community Hospital ETZ Florida Hospital Waterman CTZ Shawnee Mission Medical Center
AUTHORIZED PAYER ACCESS LIAISON SIGNATURE: ______Date: ______
*OPID: ______*COST CENTER: ______
*To be completed by AHS