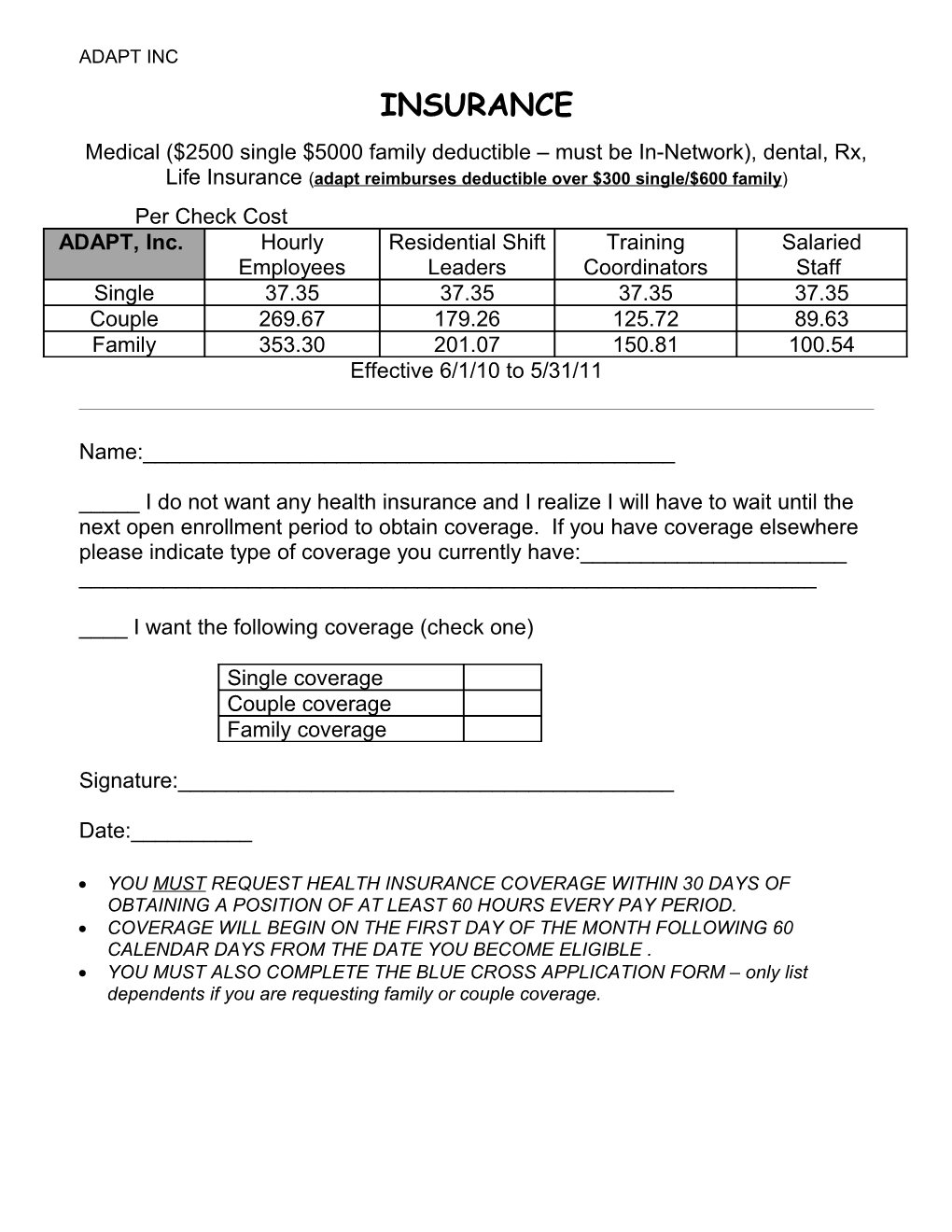
ADAPT INC INSURANCE Medical ($2500 single $5000 family deductible – must be In-Network), dental, Rx, Life Insurance (adapt reimburses deductible over $300 single/$600 family) Per Check Cost ADAPT, Inc. Hourly Residential Shift Training Salaried Employees Leaders Coordinators Staff Single 37.35 37.35 37.35 37.35 Couple 269.67 179.26 125.72 89.63 Family 353.30 201.07 150.81 100.54 Effective 6/1/10 to 5/31/11
Name:______
_____ I do not want any health insurance and I realize I will have to wait until the next open enrollment period to obtain coverage. If you have coverage elsewhere please indicate type of coverage you currently have:______
____ I want the following coverage (check one)
Single coverage Couple coverage Family coverage
Signature:______
Date:______
YOU MUST REQUEST HEALTH INSURANCE COVERAGE WITHIN 30 DAYS OF OBTAINING A POSITION OF AT LEAST 60 HOURS EVERY PAY PERIOD. COVERAGE WILL BEGIN ON THE FIRST DAY OF THE MONTH FOLLOWING 60 CALENDAR DAYS FROM THE DATE YOU BECOME ELIGIBLE . YOU MUST ALSO COMPLETE THE BLUE CROSS APPLICATION FORM – only list dependents if you are requesting family or couple coverage.