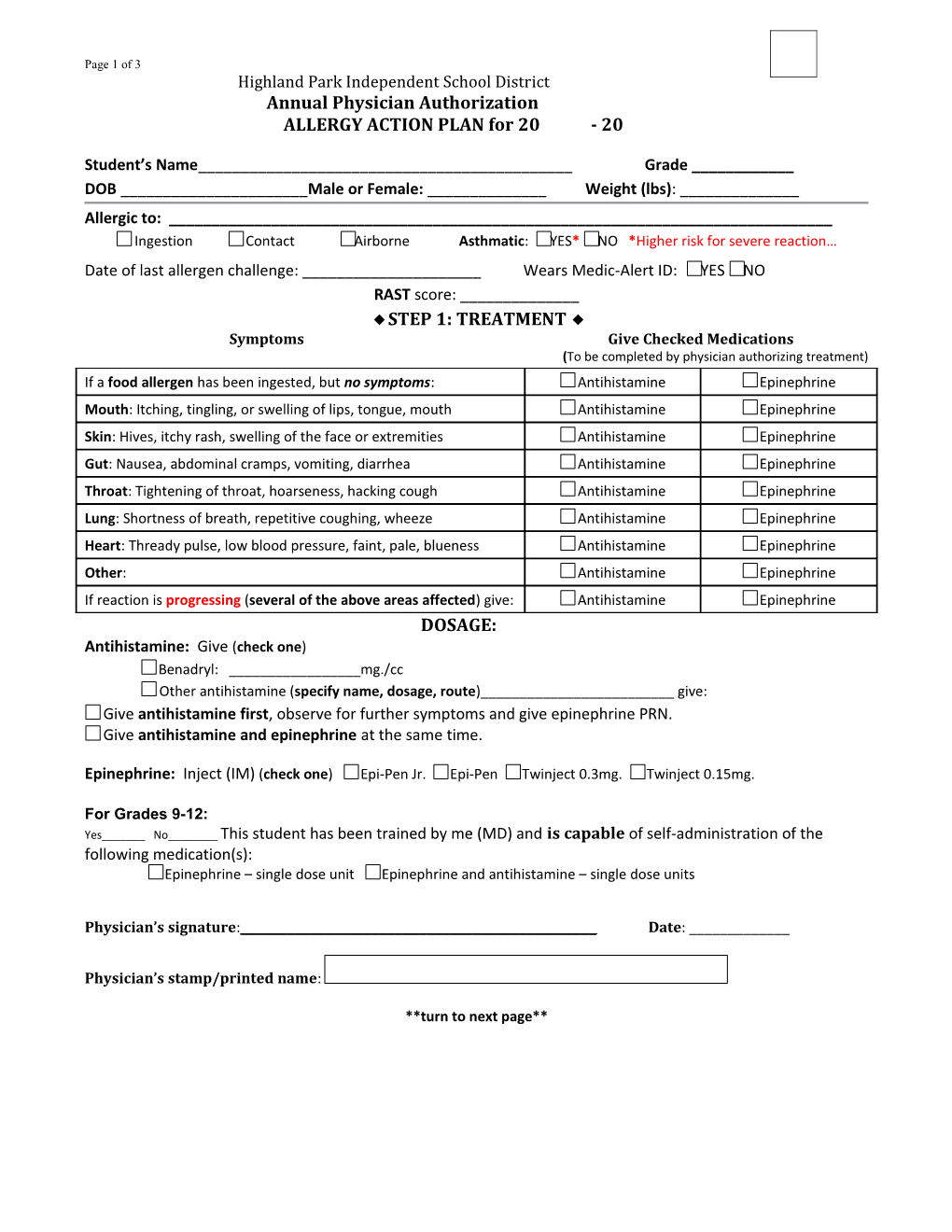
Page 1 of 3 Highland Park Independent School District Annual Physician Authorization ALLERGY ACTION PLAN for 20 - 20
Student’s Name______Grade ______DOB ______Male or Female: ______Weight (lbs): ______Allergic to: ______Ingestion Contact Airborne Asthmatic: YES* NO *Higher risk for severe reaction… Date of last allergen challenge: ______Wears Medic-Alert ID: YES NO RAST score: ______◆ STEP 1: TREATMENT ◆ Symptoms Give Checked Medications (To be completed by physician authorizing treatment) If a food allergen has been ingested, but no symptoms: Antihistamine Epinephrine Mouth: Itching, tingling, or swelling of lips, tongue, mouth Antihistamine Epinephrine Skin: Hives, itchy rash, swelling of the face or extremities Antihistamine Epinephrine Gut: Nausea, abdominal cramps, vomiting, diarrhea Antihistamine Epinephrine Throat: Tightening of throat, hoarseness, hacking cough Antihistamine Epinephrine Lung: Shortness of breath, repetitive coughing, wheeze Antihistamine Epinephrine Heart: Thready pulse, low blood pressure, faint, pale, blueness Antihistamine Epinephrine Other: Antihistamine Epinephrine If reaction is progressing (several of the above areas affected) give: Antihistamine Epinephrine DOSAGE: Antihistamine: Give (check one) Benadryl: ______mg./cc Other antihistamine (specify name, dosage, route)______give: Give antihistamine first, observe for further symptoms and give epinephrine PRN. Give antihistamine and epinephrine at the same time.
Epinephrine: Inject (IM) (check one) Epi-Pen Jr. Epi-Pen Twinject 0.3mg. Twinject 0.15mg.
For Grades 9-12: Yes______No______This student has been trained by me (MD) and is capable of self-administration of the following medication(s): Epinephrine – single dose unit Epinephrine and antihistamine – single dose units
Physician’s signature:______Date: ______
Physician’s stamp/printed name:
**turn to next page** Page 2 of 3 Annual Parent Authorization
◆ STEP 2: EMERGENCY CALLS ◆ 1. Call 911: State that an allergic reaction has been treated, and additional epinephrine may be needed. 2. Emergency Phone Contacts: Name Relation Phone
3. Dr. ______Phone: ______Hospital Preference: ______
I, the undersigned parent/guardian of ______, request that an antihistamine and/or epinephrine be administered to my child, as prescribed by the physician. I understand that the School Nurse would perform this procedure. It is my understanding that if the School Nurse is not available the Principal will designate appropriate staff to perform this procedure. I am aware that all staff members are trained annually on LTAs and emergency epinephrine administration. I will notify the school immediately if the health status of my child changes, if I change physicians, or if the procedure is canceled or changed in any way. I also give my consent to the school nurse to contact the physician or healthcare provider for additional information if needed. In addition, I will provide a current Epinephrine auto-injector for my child’s use. I understand that all Antihistamine and/or Epinephrine must be brought to school by an adult and be provided in the original container.
For Grades 9-12 ONLY: My child will keep epinephrine auto injection in his/her: Backpack Purse Locker Other ______
Parent’s signature: ______Date: ______
Monitoring Stay with the student; alert school nurse and parent. Tell EMS epinephrine was given; request an ambulance with epinephrine. Note time with epinephrine was administered. A second dose of epinephrine can be given 5 minutes or more after the first if symptoms persist or recur. For a severe reaction, consider keeping student lying on back with legs raised. Page 3 of 3 Highland Park Independent School District Health Services Severe Food Allergy Questionnaire
Dear Parent/Guardian,
Thank you for completing this questionnaire regarding your child’s severe food allergy. This information is important for the nurse to have in order for her/him to develop an individualized healthcare plan for your child and is used to coordinate the safe care of your child while at school.
Student: ______DOB: ______Male Female
Severe Allergy: ______
Has your child been diagnosed with asthma or eczema in addition to a severe allergy?
Asthma Eczema Neither
What age was the allergy first noted? ______When was your child’s last reaction? ______
Has your child ever received an epinephrine injection (such as an Epi Pen) during an allergic reaction? Yes No
When was the last time the physician tested your child’s sensitivity level to the allergen? ______
What type of exposure is necessary for an allergic reaction to occur? Ingestion Contact Inhalation
Does your child know when he/she is having an allergic reaction, and are they able to tell an adult? Yes No
How does your child act and what do they say when they are having symptoms of an allergic reaction? ______
______
______
______
Do you feel your child has a good understanding about their allergy? ………………………………………………………… Yes No
Does your child know what foods not to eat or touch? ...... Yes No
Does your child wear an allergy alert necklace or bracelet? ……………………………………………………………………….. Yes No
Do you prefer that your child sit at a designated peanut/nut free table in the cafeteria (Elementary only)? Yes No
Is your child emotionally sensitive about his/her allergy? …………………………………………………………………………….. Yes No
Do you give us permission to notify your child’s teacher(s) about his/her allergy? ……………………………………….. Yes No
Regarding 504 Reviews – 504 reviews are required every three (3) years. However, annual meetings can still take place, if preferred. Please check the appropriate box on your preferences regarding 504 Reviews.
Every three (3) years Annually (every year)
Additional information:
______
Parent/Guardian Signature: ______Date: ______(02/17)