Appendix B: Data Abstraction Forms
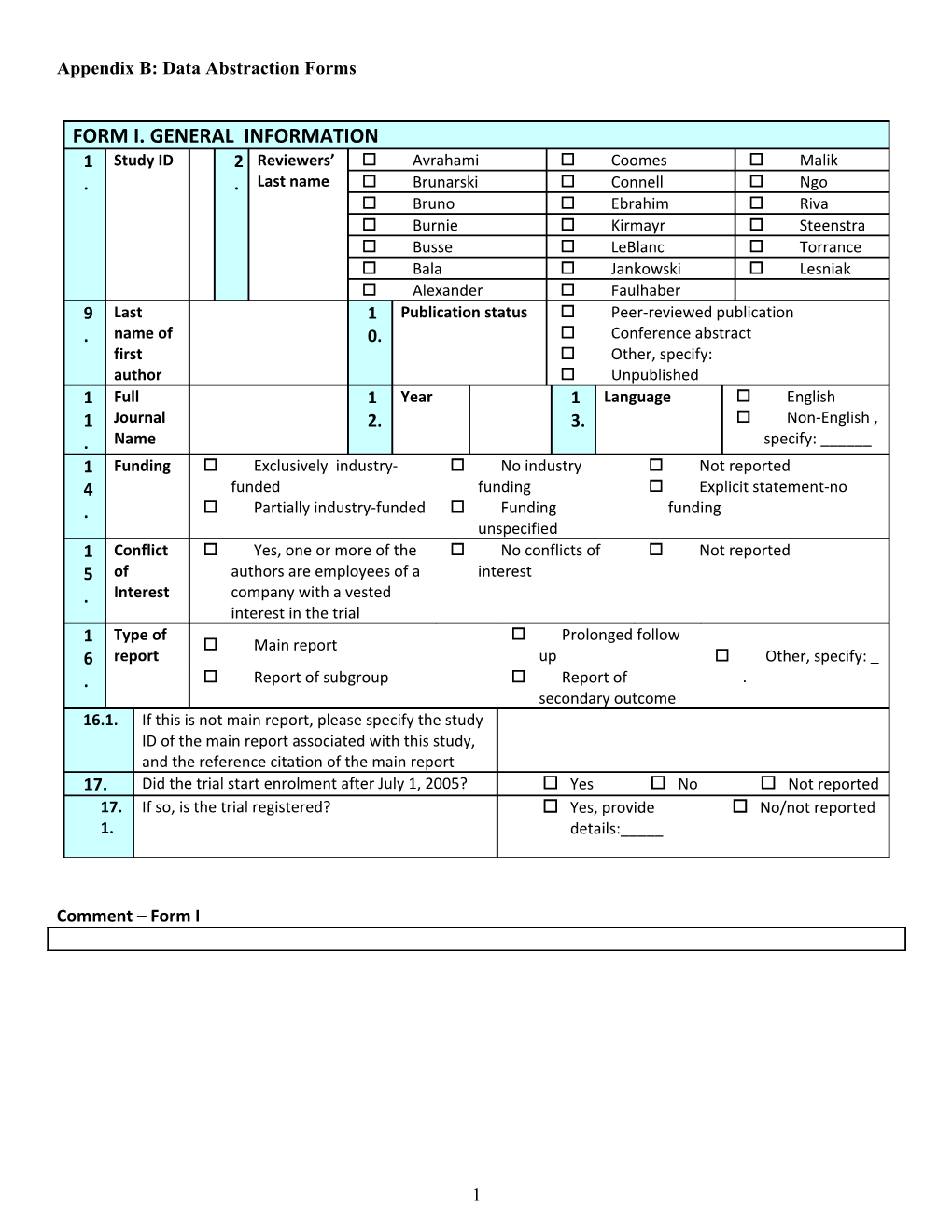
FORM I. GENERAL INFORMATION 1 Study ID 2 Reviewers’ Avrahami Coomes Malik . . Last name Brunarski Connell Ngo Bruno Ebrahim Riva Burnie Kirmayr Steenstra Busse LeBlanc Torrance Bala Jankowski Lesniak Alexander Faulhaber 9 Last 1 Publication status Peer-reviewed publication . name of 0. Conference abstract first Other, specify: author Unpublished 1 Full 1 Year 1 Language English 1 Journal 2. 3. Non-English , . Name specify: ______1 Funding Exclusively industry- No industry Not reported 4 funded funding Explicit statement-no . Partially industry-funded Funding funding unspecified 1 Conflict Yes, one or more of the No conflicts of Not reported 5 of authors are employees of a interest . Interest company with a vested interest in the trial Type of Prolonged follow 1 Main report 6 report up Other, specify: . Report of subgroup Report of . secondary outcome 16.1. If this is not main report, please specify the study ID of the main report associated with this study, and the reference citation of the main report 17. Did the trial start enrolment after July 1, 2005? Yes No Not reported 17. If so, is the trial registered? Yes, provide No/not reported 1. details:_____
Comment – Form I
1 FORM II. STUDY CHARACTERISTICS 18. Where was this study conducted Canada United States Check all that apply United Kingdom Other Europe Japan Other Asia Africa Australia New Zealand South America Not reported 19. Number of sites Single site 2-5 sites 6-10 sites > 10 sites Not reported 20. Study design Parallel trial Cross-over trial Factorial trial N-of-1 trial Cluster trial 21. Primary outcome(s) Specified: ______ Not specified 22. Number of applicable arms 2 3 4 Other, specify 23. Number of individual approached to take part in the Reported, specify: ______study who chose not to participate Not reported 24. Did the trial authors implement a pre-randomization Yes period? No 24. If so, what reason was provided? To establish severity and variability of pain 1. To identify and exclude patients with high responses to placebo (placebo run-in period) To identify and exclude patients with intolerable side effects to study treatment (active treatment run-in period) To treat all patients with the active therapy, and then only randomize responders To identify and exclude on-adherent patients Other reason (specify)
2 FORM II. STUDY CHARACTERISTICS - continued 25. Was involvement in litigation reported? Yes No Unclear 25. If so, was involvement in litigation used as exclusion Yes 1. criteria? No
26. Was receipt of disability benefits or other wage Yes replacement benefits reported? No Unclear 26. If so, was receipt of disability benefits or other wage Yes 1. replacement benefits used as exclusion criteria? No
27. Duration of treatment (check 1 only) Days:______ Weeks: ______ Months: ______ Years: ______28. Frequency of treatment (check 1 only) Not applicable Times per day: ______ Times per week: ______ Times per month: ______29. Duration of the individual treatment unit (check 1 Not applicable only) Minutes: ______ Hours: ______ Other, specify: ______30. Length of follow up from randomization Fixed period → (expand if selected) Variable period (complete all the following as appropriate) → Minimum (expand if selected) → Maximum (expand if selected) → Median (expand if selected) → Mean (expand if selected) → Person years .
Comment – Form II
3 FORM III. RISK OF BIAS
4 3 How was the Computer generated randomization scheme 2 randomization sequence Random number table . generated? Tossing coin Rolling of a dice Picking allocation from a hat/box Minimization/dynamic allocation Other, specify . Not reported 3 Was allocation adequately Definitely yes 3 concealed? Probably yes . Probably no Definitely no 3 How was allocation Sequentially numbered, opaque, sealed envelope 4 concealed? Sequentially coded medication containers . Central randomization (including telephone, web-based and pharmacy-controlled randomization); Open random allocation schedule(open-label) “Concealed”, no method described Other, specify : ______ Not concealed Not reported 3 Blinding of patients 5 Definitely yes Probably yes Probably no Definitely no . 3 Blinding of health Care 6 providers Definitely yes Probably yes Probably no Definitely no . 3 Blinding of data collectors 7 Definitely yes Probably yes Probably no Definitely no . 3 Blinding of outcome 8 assessors Definitely yes Probably yes Probably no Definitely no . 3 Blinding of data analysts 9 Definitely yes Probably yes Probably no Definitely no . 4 Study stopped early for Yes No No clear statement 0 benefit . 4 Study stopped early for Yes No No clear statement 1 harm . 4 Whether patients were 2 analyzed in the groups to Yes No Not reported . which they were randomized?
5 FORM III. RISK OF BIAS - continued 1 Lost to follow up (LTFU) explicitly Explicit Explicit statement: No explicit . reported statement: LTFU LTFU did not occur statement about occurred LTFU 2 LTFU reported separately for Yes No No explicit . each study arm statement about LTFU 3 LTFU reported relative to each Yes No N/A (only one . planned follow-up planned) N/A (no LTFU) 4 Implications of LTFU discussed Yes No N/A . 5 Method of dealing with LTFU Yes (open table No N/A . explicitly described below)
Comment – Form III
FORM IV. INTERVENTIONS 4 Treatment Arm 1 Analgesic: code ______3. (check all that apply) Anesthetic: code ______ Anticonvulsant: code ______ Anti-Depressant: code ______ Anti-Emetic: code ______
Anti-hypertensive: code ______ Anti-Inflammatory: code ______ Anti-Viral: code ______
Bone Growth Stimulant: code ______ Complementary & Alternative Therapy: code ______ Dopamine Agonist: code ______ Exercise: code ______ Hormone Therapy: code ______ Immunological Modifier: code ______ Lifestyle Modification: code ______ Muscle Relaxant: code ______ Nutrition & Supplements: code ______ Psychotherapy: code ______ Sedative: code ______ Serotonin Antagonist: code ______ Stimulant: code ______
6 FORM IV. INTERVENTIONS 6 Treatment Arm 2 Analgesic: code ______4. (check all that apply) Anesthetic: code ______ Anticonvulsant: code ______ Anti-Depressant: code ______ Anti-Emetic: code ______
Anti-hypertensive: code ______ Anti-Inflammatory: code ______ Anti-Viral: code ______
Bone Growth Stimulant: code ______ Complementary & Alternative Therapy: code ______ Dopamine Agonist: code ______ Exercise: code ______ Hormone Therapy: code ______ Immunological Modifier: code ______ Lifestyle Modification: code ______ Muscle Relaxant: code ______ Nutrition & Supplements: code ______ Psychotherapy: code ______ Sedative: code ______ Serotonin Antagonist: code ______ Stimulant: code ______
7 FORM IV. INTERVENTIONS 8 Treatment Arm 3 Analgesic: code ______5. (check all that apply) Anesthetic: code ______ Anticonvulsant: code ______ Anti-Depressant: code ______ Anti-Emetic: code ______
Anti-hypertensive: code ______ Anti-Inflammatory: code ______ Anti-Viral: code ______
Bone Growth Stimulant: code ______ Complementary & Alternative Therapy: code ______ Dopamine Agonist: code ______ Exercise: code ______ Hormone Therapy: code ______ Immunological Modifier: code ______ Lifestyle Modification: code ______ Muscle Relaxant: code ______ Nutrition & Supplements: code ______ Psychotherapy: code ______ Sedative: code ______ Serotonin Antagonist: code ______ Stimulant: code ______
8 FORM IV. INTERVENTIONS 1 Control Arm Analgesic: code ______0 (check all that apply) 6. Anesthetic: code ______ Anticonvulsant: code ______ Anti-Depressant: code ______ Anti-Emetic: code ______
Anti-hypertensive: code ______ Anti-Inflammatory: code ______ Anti-Viral: code ______
Bone Growth Stimulant: code ______ Complementary & Alternative Therapy: code ______ Dopamine Agonist: code ______ Exercise: code ______ Hormone Therapy: code ______ Immunological Modifier: code ______ Lifestyle Modification: code ______ Muscle Relaxant: code ______ Nutrition & Supplements: code ______ Placebo Psychotherapy: code ______ Sedative: code ______ Serotonin Antagonist: code ______ Stimulant: code ______ Waiting List
Comment – Form IV
9 Form V: PATIENT CHARACTERISTICS
1 What clinical conditions were studied? Fibromyalgia 2 Generalized myofascial pain syndrome 9 Fibrositis . Muscular rheumatism Chronic, generalized pain syndrome 1 Were explicit criteria used to identify participants? Unequivocal clear and explicit criteria 3 Some criteria, but not as clear or explicit as desirable 0 Uncertain . Not reported Reported in a prior publication 1 Did ≥50% of participants clearly meet the diagnostic Yes 3 criteria for fibromyalgia according to the American No 1 College of Rheumatology [ACR] criteria, 1990? Uncertain . Measure Tx Group 1 Tx Group 2 Tx Group 3 Control Arm Total
10 1 Duration of chronic pain condition , , , , , 3 before randomization (in years) Mean, SD . . . . . 2 Not reported , , , , , . Median, IQR . . . . . 1 Age (year) , , , , , 3 Not reported Mean, SD . . . . . 4 , , , , , . Median, IQR . . . . . 1 Number of female participants 3 Not reported 6 . Raw number 1 Involved in litigation 3 Not reported 7 . Raw number 1 Receiving disability or other wage 3 replacement benefits 8 Not reported . Raw number 1 Intensity of required participation 3 9 High High High High High . Low Low Low Low Low 1 Compliance with treatment 4 Not reported 0 . Percentage
Comment – Form V
11 FORM VI: PARTICIPANT FLOW THROUGH STUDY Tx Group 1 Tx Group 2 Tx Group 3 Control arm Total 14 Patients randomized (raw number) 1. Not reported
14 Patients mistakenly randomized, appropriately 2. excluded (raw number) Not reported 14 Patients mistakenly randomized, 3. inappropriately excluded (raw number) Not reported 14 Lost to follow-up: withdrew consent (raw 4. number) Not reported 14 Lost to follow-up: withdrew due to adverse 5. effects (raw number) Not reported 14 Lost to follow-up: withdrew due to lack of 6. improvement (raw number) Not reported 14 Lost to follow-up: withdrew due to loss of 7. contact or migration (raw number) Not reported 14 Lost to follow-up: withdrew due to Other 8. Reasons (raw number) Not reported
12 FORM VII: OUTCOMES
149. Binary Outcome Number of events / total (denominator) Reported Tx Group 1 Tx Group 2 Tx Group 3 Control Arm Not reported → skip this table Events Total Person- Events Total Person- Events Total Person- Events Total Person- years years years years Total Outcome Code Is the Endpoint a threshold? Yes (describe) No Is a higher risk better or worse? Higher risk is better Higher risk is worse Follow-up time Days: ______ Weeks: ______ Months: ______ Years: ______Effect estimates Reported Not reported → skip to next outcome Effect measure RR OR HR ARR/RD Effect estimates Point estimate (95% CI) Unadjusted analyses Adjusted analyses Group 1 vs. Group 2 Group 1 vs. Group 3 Group 1 vs. Control Arm Group 2 vs. Group 3 Group 2 vs. Control Arm Group 3 vs. Control Arm
13 150. Continuous Score Outcome Tx Group 1 Tx Group 2 Tx Group 3 Control Arm Reported Not reported → skip this table Unit of measure Unitless Specific unit of measure: ______Measure of central Mean Median Mode tendency Measure of variance Unit of variance measure SD SE 95% IQR range CI Outcome Code Is a higher score better or Higher score is better Higher score is worse worse? Follow-up time Days: Weeks: Months: Years: ______Number of patients available for analysis
Comment – Form VI
14