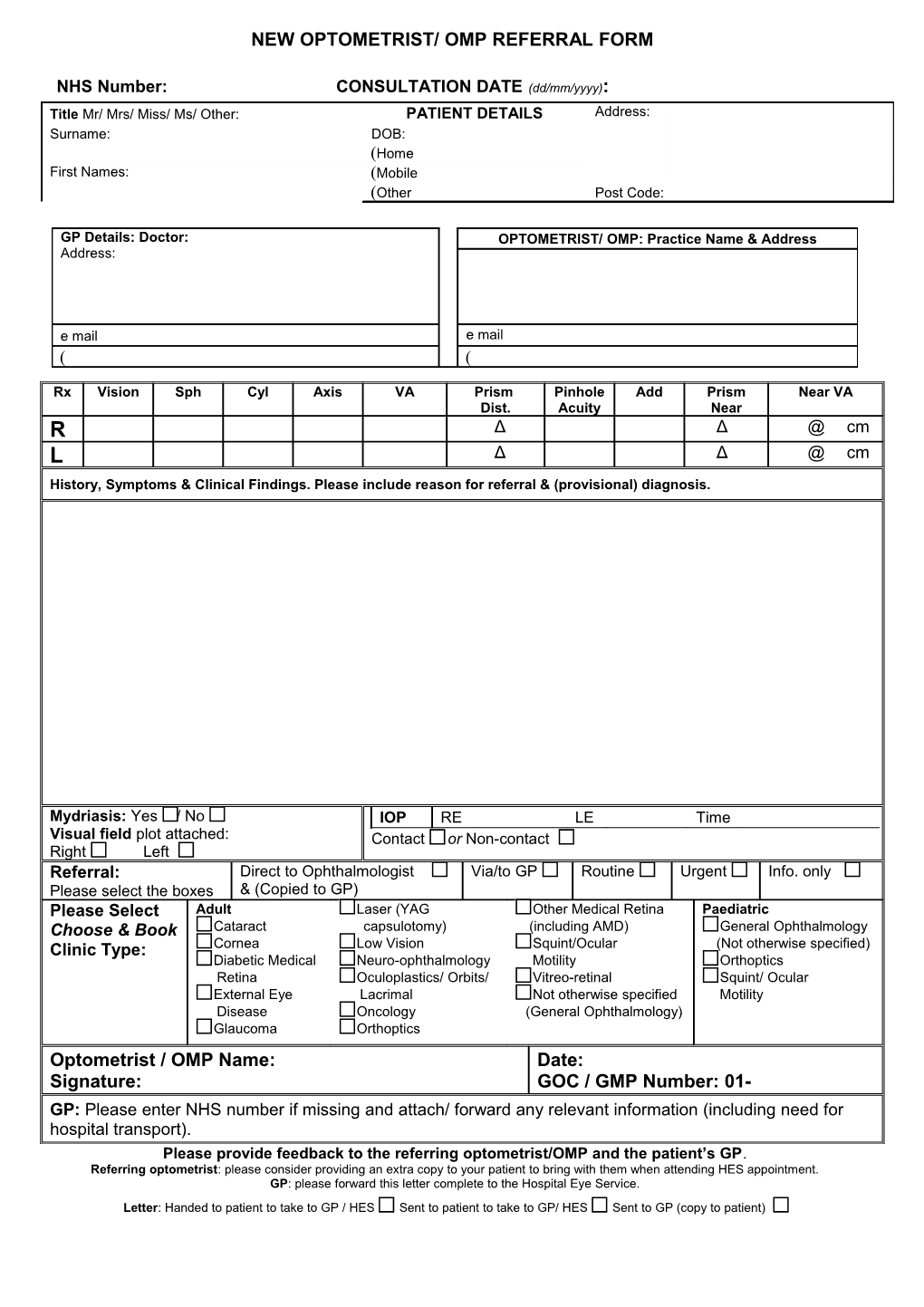
NEW OPTOMETRIST/ OMP REFERRAL FORM
NHS Number: CONSULTATION DATE (dd/mm/yyyy): Title Mr/ Mrs/ Miss/ Ms/ Other: PATIENT DETAILS Address: Surname: DOB: Home First Names: Mobile Other Post Code:
GP Details: Doctor: OPTOMETRIST/ OMP: Practice Name & Address Address:
e mail e mail
Rx Vision Sph Cyl Axis VA Prism Pinhole Add Prism Near VA Dist. Acuity Near R Δ Δ @ cm L Δ Δ @ cm History, Symptoms & Clinical Findings. Please include reason for referral & (provisional) diagnosis.
Mydriasis: Yes / No IOP RE LE Time Visual field plot attached: Contact or Non-contact Right Left Referral: Direct to Ophthalmologist Via/to GP Routine Urgent Info. only Please select the boxes & (Copied to GP) Please Select Adult Laser (YAG Other Medical Retina Paediatric Choose & Book Cataract capsulotomy) (including AMD) General Ophthalmology Clinic Type: Cornea Low Vision Squint/Ocular (Not otherwise specified) Diabetic Medical Neuro-ophthalmology Motility Orthoptics Retina Oculoplastics/ Orbits/ Vitreo-retinal Squint/ Ocular External Eye Lacrimal Not otherwise specified Motility Disease Oncology (General Ophthalmology) Glaucoma Orthoptics Optometrist / OMP Name: Date: Signature: GOC / GMP Number: 01- GP: Please enter NHS number if missing and attach/ forward any relevant information (including need for hospital transport). Please provide feedback to the referring optometrist/OMP and the patient’s GP. Referring optometrist: please consider providing an extra copy to your patient to bring with them when attending HES appointment. GP: please forward this letter complete to the Hospital Eye Service. Letter: Handed to patient to take to GP / HES Sent to patient to take to GP/ HES Sent to GP (copy to patient)