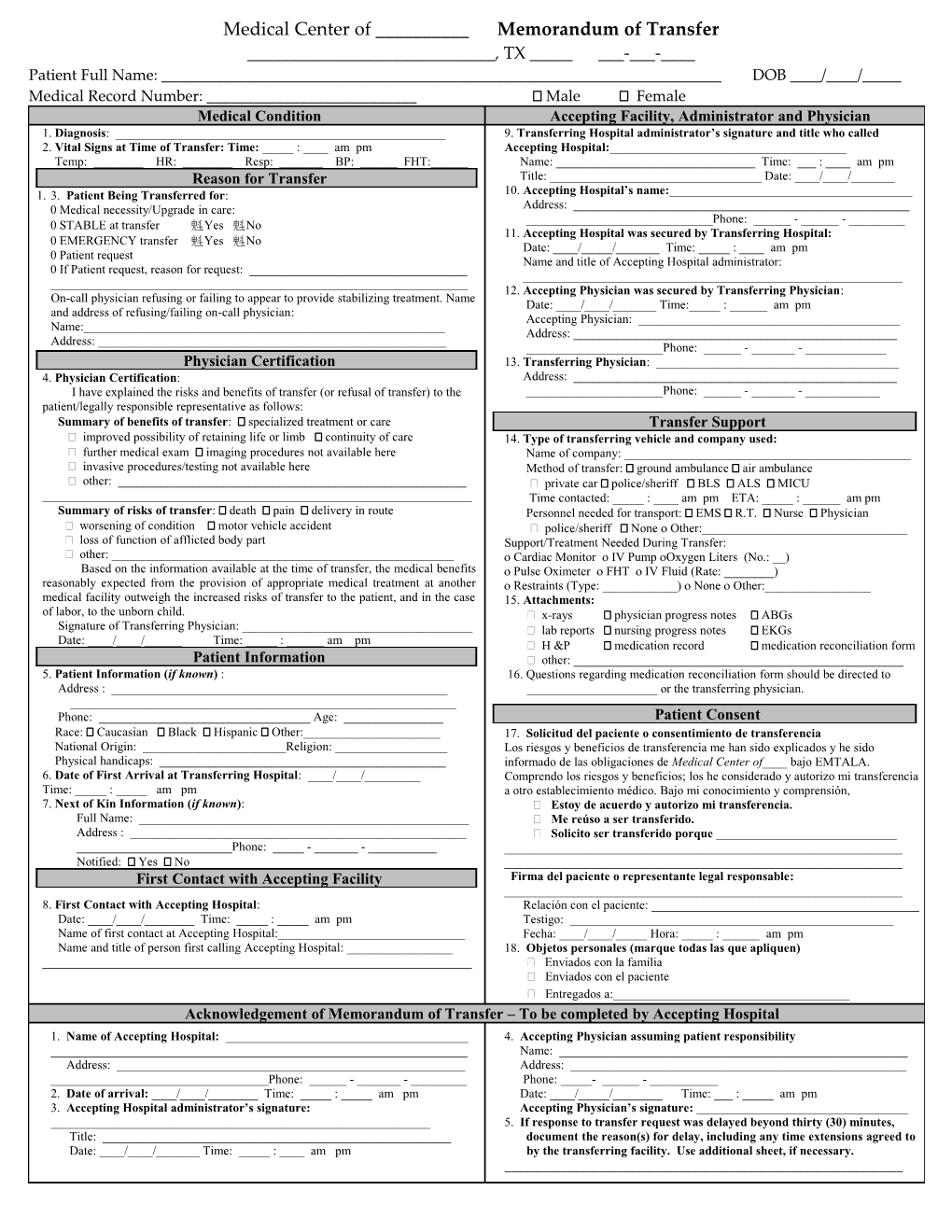
Medical Center of ______Memorandum of Transfer ______, TX ______-___-____ Patient Full Name: ______DOB ____/____/_____ Medical Record Number: ______ Male Female Medical Condition Accepting Facility, Administrator and Physician 1. Diagnosis: ______9. Transferring Hospital administrator’s signature and title who called 2. Vital Signs at Time of Transfer: Time: _____ : ____ am pm Accepting Hospital:______Temp: ______HR: ______Resp: ______BP: ______FHT:______Name: ______Time: ___ : ____ am pm Reason for Transfer Title: ______Date: ____/____/______1. 3. Patient Being Transferred for: 10. Accepting Hospital’s name:______ Medical necessity/Upgrade in care: Address: ______Phone: ______- ______- ______ STABLE at transfer Yes No 11. Accepting Hospital was secured by Transferring Hospital: EMERGENCY transfer Yes No Date: ____/_____/______Time: _____ : ____ am pm Patient request Name and title of Accepting Hospital administrator: If Patient request, reason for request: ______12. Accepting Physician was secured by Transferring Physician: On-call physician refusing or failing to appear to provide stabilizing treatment. Name Date: ____/____/______Time:_____ : ______am pm and address of refusing/failing on-call physician: Accepting Physician: ______Name:______Address: ______Address: ______Phone: ______- ______- ______Physician Certification 13. Transferring Physician: ______4. Physician Certification: Address: ______I have explained the risks and benefits of transfer (or refusal of transfer) to the ______Phone: ______- ______- ______patient/legally responsible representative as follows: Summary of benefits of transfer: specialized treatment or care Transfer Support improved possibility of retaining life or limb continuity of care 14. Type of transferring vehicle and company used: further medical exam imaging procedures not available here Name of company: ______ invasive procedures/testing not available here Method of transfer: ground ambulance air ambulance other: ______ private car police/sheriff BLS ALS MICU ______Time contacted: _____ : ____ am pm ETA: _____ : ______am pm Summary of risks of transfer: death pain delivery in route Personnel needed for transport: EMS R.T. Nurse Physician worsening of condition motor vehicle accident police/sheriff None Other:______ loss of function of afflicted body part Support/Treatment Needed During Transfer: other: ______ Cardiac Monitor IV Pump Oxygen Liters (No.: __) Based on the information available at the time of transfer, the medical benefits Pulse Oximeter FHT IV Fluid (Rate: ______) reasonably expected from the provision of appropriate medical treatment at another Restraints (Type: ______) None Other:______medical facility outweigh the increased risks of transfer to the patient, and in the case 15. Attachments: of labor, to the unborn child. x-rays physician progress notes ABGs Signature of Transferring Physician: ______ lab reports nursing progress notes EKGs Date: ____/____/______Time: _____ : ______am pm H &P medication record medication reconciliation form Patient Information other: ______5. Patient Information (if known) : 16. Questions regarding medication reconciliation form should be directed to Address : ______or the transferring physician. ______Phone: ______Age: ______Patient Consent Race: Caucasian Black Hispanic Other:______17. Solicitud del paciente o consentimiento de transferencia National Origin: ______Religion: ______Los riesgos y beneficios de transferencia me han sido explicados y he sido Physical handicaps: ______informado de las obligaciones de Medical Center of____ bajo EMTALA. 6. Date of First Arrival at Transferring Hospital: ____/____/______Comprendo los riesgos y beneficios; los he considerado y autorizo mi transferencia Time: _____ : _____ am pm a otro establecimiento médico. Bajo mi conocimiento y comprensión, 7. Next of Kin Information (if known): Estoy de acuerdo y autorizo mi transferencia. Full Name: ______ Me reúso a ser transferido. Address : ______ Solicito ser transferido porque ______Phone: _____ - ______- ______Notified: Yes No ______First Contact with Accepting Facility Firma del paciente o representante legal responsable: ______8. First Contact with Accepting Hospital: Relación con el paciente: ______Date: ____/____/______Time: _____ : _____ am pm Testigo: ______Name of first contact at Accepting Hospital:______Fecha: ____/____/_____ Hora: _____ : ______am pm Name and title of person first calling Accepting Hospital: ______18. Objetos personales (marque todas las que apliquen) ______ Enviados con la familia Enviados con el paciente Entregados a:______Acknowledgement of Memorandum of Transfer – To be completed by Accepting Hospital 1. Name of Accepting Hospital: ______4. Accepting Physician assuming patient responsibility ______Name: ______Address: ______Address: ______Phone: ______- ______- ______Phone: _____- ______- ______2. Date of arrival: ____/____/______Time: _____ : _____ am pm Date: ____/_____/______Time: ___ : _____ am pm 3. Accepting Hospital administrator’s signature: Accepting Physician’s signature: ______5. If response to transfer request was delayed beyond thirty (30) minutes, Title: ______document the reason(s) for delay, including any time extensions agreed to Date: ____/____/______Time: _____ : ____ am pm by the transferring facility. Use additional sheet, if necessary. ______
SECTION A: to Be Completed by Transferring Hospital
Total Page:16
File Type:pdf, Size:1020Kb
Recommended publications