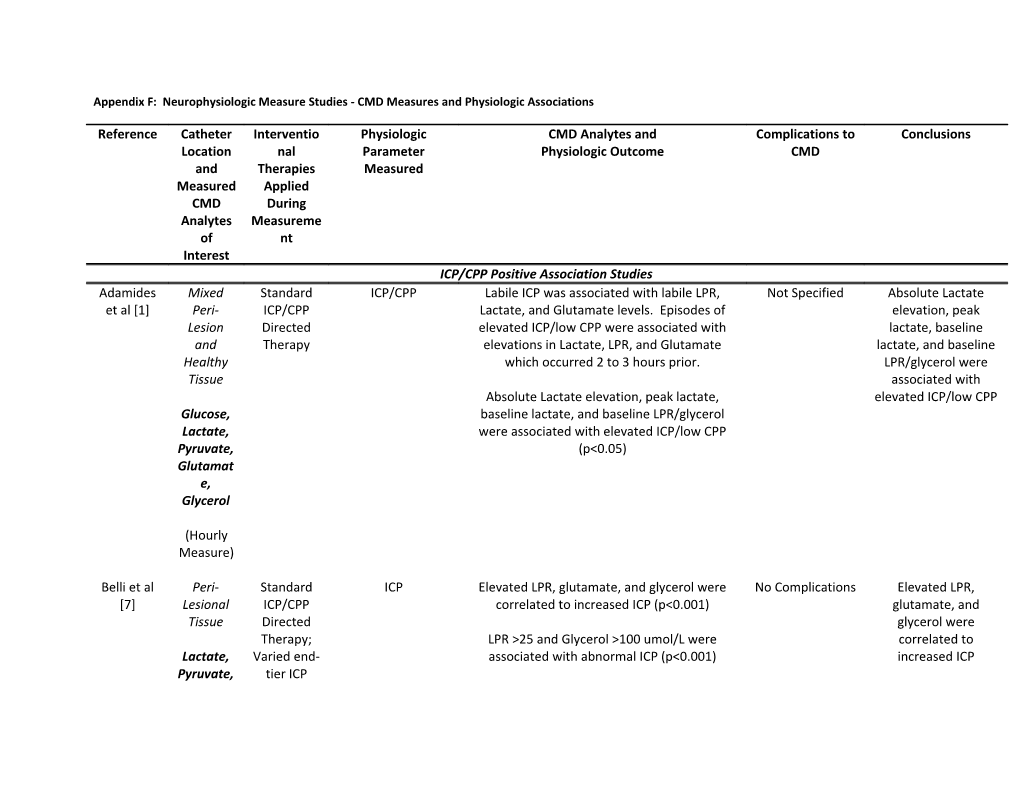
Appendix F: Neurophysiologic Measure Studies - CMD Measures and Physiologic Associations
Reference Catheter Interventio Physiologic CMD Analytes and Complications to Conclusions Location nal Parameter Physiologic Outcome CMD and Therapies Measured Measured Applied CMD During Analytes Measureme of nt Interest ICP/CPP Positive Association Studies Adamides Mixed Standard ICP/CPP Labile ICP was associated with labile LPR, Not Specified Absolute Lactate et al [1] Peri- ICP/CPP Lactate, and Glutamate levels. Episodes of elevation, peak Lesion Directed elevated ICP/low CPP were associated with lactate, baseline and Therapy elevations in Lactate, LPR, and Glutamate lactate, and baseline Healthy which occurred 2 to 3 hours prior. LPR/glycerol were Tissue associated with Absolute Lactate elevation, peak lactate, elevated ICP/low CPP Glucose, baseline lactate, and baseline LPR/glycerol Lactate, were associated with elevated ICP/low CPP Pyruvate, (p<0.05) Glutamat e, Glycerol
(Hourly Measure)
Belli et al Peri- Standard ICP Elevated LPR, glutamate, and glycerol were No Complications Elevated LPR, [7] Lesional ICP/CPP correlated to increased ICP (p<0.001) glutamate, and Tissue Directed glycerol were Therapy; LPR >25 and Glycerol >100 umol/L were correlated to Lactate, Varied end- associated with abnormal ICP (p<0.001) increased ICP Pyruvate, tier ICP LPR, therapies Glutamat (DC, etc.) e
(q12 Hour Measure)
Bolcha et al Unclear Not ICP and PbtO2 ICP: High ICP was associated with high LPR and Not Specified High LPR and Glycerol [10] Location Specified Glycerol are associated with high ICP. High LPR is
Glucose, PbtO2: High LPR correlated with low PbtO2 associated with low
Glycerol, PbtO2. LPR
(Unclear Interval)
Bullock et Mixed Standard ICP/CPP High Glutamate (>20 umol/L) was associated 3 catheters High Glutamate is al [12] Peri- ICP with elevated ICP/low CPP (p=0.0104) malfunctioned associated with Lesion Therapy; requiring elevated ICP and “Few” with Glutamate was linearly correlated to the replacement Healthy barbiturate severity of secondary ischemic episodes
Tissue infusions (defined by ischemia score; PaO2, MABP, Xe CT, pupil response, CPP) (p=0.025) Glutamat e
(q30 min Measure for 4 days)
Clausen et Healthy Various ICP CPP and PbtO2 PbtO2: Glycerol levels negatively correlated Not Specified High Glycerol levels
al [17] Tissue Therapies with PbtO2 (p<0.001) are associated with low PbtO2 and low Glycerol CPP: Glycerol levels negatively correlated with CPP. CPP (p<0.05) (q30 min Measure)
Clausen et Healthy Various ICP CPP and PbtO2 CPP: High lactate observed in episodes of low Not Specified High Lactate is with
al [18] Tissue Therapies; CPP (mean 1027 umol/L), with the largest low CPP and PbtO2. Barbiturate mean change in lactate correlating significantly Lactate s; (p<0.05) Hypothermi
(q30 min a PbtO2: High lactate was associated with low
Measure) PbtO2. (p<0.05)
Goodman Healthy Various ICP ICP As Glutamate decreases (with progressive Not Specified Glutamate Levels are et al [26] Tissue Therapies sedation) so does ICP Associated with ICP (including Glutamat Barbiturate e s)
(q 30min Measure)
Goodman Mixed Various ICP ICP, SjVO2, PbtO2 ICP: Lactate increases and Glucose decreases Not Specified Increases in Lactate et al [25] Peri- Therapies; as ICP continuously increases and Glucose were Lesion DC associated with an
and SjvO2: Elevated Lactate (median increase increase in ICP and
Healthy >0.322 umol/L) was associated to decrease in decrease in SjvO2
Tissue SjvO2 (p=0.002). The change in Glucose was
related to the severity of SjVO2 decrease Lactate (p=0.032) and
Glucose PbtO2: Increased in Lactate did not correlate to
local changes in PbtO2. (Unclear Interval)
Gupta et al Unclear ICP/CPP ICP LPR and CPP displayed a negative correlation Not Specified Elevations in LPR are [28] Location Directed (p=0.029) associated with a Therapy decrease in CPP Glycerol, Lactate, Pyruvate, LPR
(Unclear Interval)
Hejcl et al Unclear Not ICP/CPP, PbtO2 ICP/CPP: High LPR associated with elevated ICP Not Specified High LPR is associated [34] Location Specified (p<0.05), and low CPP (p<0.05) with high ICP and low CPP/PbtO2. High Glucose, High Glycerol associated with elevated ICP Glycerol is associated Glycerol, (p<0.05) with high ICP LPR
PbtO2: High LPR was associated with low PbtO2 (Unclear (p<0.05) Interval)
Koura et al Unclear Not ICP Elevated Glutamate was associated with Not Specified High Glutamate is [47] Location Specified elevated ICP associated with ICP elevations Glutamat e
(Unclear Interval for 5 days) Kurtz et al Unclear ICP CPP and PbtO2 CPP: Low Glucose is associated with low CPP Not Specified Low glucose is [48] Location Therapies; associated with low
Hypothermi PbtO2: High LPR and Low Glucose is associated CPP/PbtO2. High LPR
Glucose, a with low PbtO2 is associated with low
Lactate, PbtO2 LPR
(Hourly Measure)
Li et al [51] Mixed Various ICP ICP/CPP and CBF ICP/CPP: High Glycerol was associated with Not Specified High Glycerol is Peri- Therapies (Laser Doppler decreased CPP and increased ICP associated with high Lesion Flowmetry) ICP and low CPP/CBF and CBF: High Glycerol was associated with Healthy reduced CBF Tissue
Glycerol
(Hourly Measure)
Meixensber Peri- Variable ICP and PbtO2 ICP: Glutamate was only associated with CMD catheter High Glutamate is ger et al Lesional Surgical and severe spikes in ICP in some cases failure in 5 sometimes associated [56] Medical with ICP spikes.
Glucose, Treatments PbtO2: Elevated LPR (>25) was associated with Elevated LPR is
Lactate, for ICP low PbtO2 (p<0.001) associated with low
Pyruvate, PbtO2. LPR, Glutamat e
(q1-2 Hour Measures)
Nelson et al Mixed ICP and CPP ICP/CPP Strong correlation between ICP/CPP and all Not Specified Low glucose, high [61] Peri-lesion directed CMD measures (ie. Low glucose, high lactate/LPR/glycerol and Therapy; lactate/LPR/glycerol seen in episodes of high seen in episodes of Healthy some with ICP/low CPP) high ICP/low CPP DC, Glucose, barbiturate Lactate, s, Pyruvate, hypothermi Glycerol a
(Hourly Measures)
Nordstrom Mixed Lund CPP Low CPP (<20 mmHg) corresponded to increase Not Specified LPR increases when et al [62] Peri- Therapy in LPR CPP drops Lesion dramatically and Healthy Tissue
Glucose, Lactate, Glutamat e, Glycerol
(Hourly Measure)
Papanikola Unclear Not ICP Elevated Glycerol predicted ICP increase Not Specified Lactate, Pyruvate, LPR ou et al Location Specified and Glycerol do not [68] correlate with Lactate, outcome Pyruvate, LPR, Glycerol
(Unclear Interval)
Paraforou Peri- ICP ICP High LPR and Glycerol occurred during times of Not Specified High LPR and Glycerol et al [69] Lesional Directed sustained ICP elevations may be seen in Therapy circumstances of Glucose, elevated ICP Glycerol, Pyruvate, Lactate
(q2 hour Measure)
Richards et Healthy ICP ICP Mean glutamate levels positively correlated to Not Specified Glutamate at 12h and al [75] Tissue Therapies ICP (p<0.05) 24h post injury correlate to outcome Glutamat No significant correlation between hourly at 3 months e glutamate and ICP/CPP/MABP/CVP
(Hourly Measure)
Salci et al Unclear Non- ICP and Compliance High LPR correlates with High ICP and Poor Not Specified High LPR is associated [79] Location specific Compliance (p<0.0001) to increased ICP and therapies poor compliance Lactate, directed at Pyruvate, ICP/CPP LPR (Unclear Interval)
Sarrafzade Healthy Not ICP, SjvO2 and ICP: High ICP (>20 mm Hg) was associated with Not Specified High Glutamate is h et al [82] Tissue Specified PbtO2 a 4-5 fold increase in Glutamate associated with high ICP and low
Glucose, SjvO2: Low SjvO2 was associated with elevated SjvO2/PbtO2. High Lactate, Glutamate, Lactate, and Glycerol Lactate and Glycerol is Glycerol, associated with low
Glutamat PbtO2: Low PbtO2 was associated with elevated SjvO2/PbtO2 e Glutamate, Lactate, and Glycerol
(Hourly Measure)
Singla et al Unclear Not ICP LPR and Glycerol levels increase as CPP Not Specified LPR and Glycerol [86] Location Specified decreased levels increase as ICP increases LPR
(Unclear Interval)
Stahl et al Mixed Varied ICP As ICP progressively increases towards Not Specified As ICP increases to [87] Uni- and Failed ICP herniation, Glycerol/Glutamate/LPR increase herniation, Bilateral Therapies and Glucose decreases Glycerol/Glutamate/L in Peri- PR increase, while Lesion Glucose decreases and Healthy Tissue
Lactate, Pyruvate, Glutamat e, Glycerol
(q30-60 min Measure)
Stein et al Unclear Unclear ICU ICP Metabolic crisis (LPR>40) was associated with Not Specified Elevated LPR may be [89] Location protocols elevated ICP associated with sustained ICP Glucose, elevations Lactate, Pyruvate
(Unclear Interval for 7 days)
Stiefel et al Unclear Not CPP Impaired Metabolism (LPR>25) was found in Not Specified Elevated LPR (>25) [91] Location Specified associated with abnormal MMM (varied may be found in techniques; CPP, NIRS, PbtO2) episodes of abnormal Lactate, MMM Pyruvate, LPR
(Hourly Measure for 3 days)
Timofeev Mixed Not ICP and PRx ICP: Glutamate, Glycerol and LPR were found Not Specified Elevated Glutamate, et al [93] Peri-lesion Specified to elevated in those with high mean ICP values Glycerol and LPR may and be seen in those with Healthy PRx: Glutamate, Glycerol and LPR were found high ICP and Tissue to be elevated in those with positive PRx values abnormal PRx
Glucose, Lactate, Pyruvate, Glutamat e, Glycerol, LPR
(Hourly Measure)
Timofeev Unclear Not ICP/CPP, PRx, PbtO2 ICP/CPP: Increased LPR was seen with an Not Specified Increased LPR may be et al [94] Location Specified increase in ICP and decrease in CPP seen in settings of High ICP, low
Lactate, PRx: Increased LPR was associated with CPP/PbtO2, and Pyruvate, abnormal PRx abnormal PRx LPR
PbtO2: Increased LPR was seen in the setting of
(Unclear low PbtO2 Interval)
Vespa et al Unclear Standard ICP/CPP Glutamate elevations (>20 uM) were seen in No complications Glutamate elevations [98] Location ICP/CPP episodes of decreased CPP (p<0.001) and (>20 uM) may be seen Directed increased ICP at various time points during in episodes of Glutamat Therapy; admission decreased CPP and e Barbiturate elevated ICP s (Hourly intermittent Measure; ly 9 days) PbtO2/SjvO2 Positive Association Studies
Chan et al Unclear Not SjvO2 Rapid increase in Glutamate, Glycerol and Not Specified Increase in [15] Location Specified Lactate were ween with SjvO2 levels below 40 Glutamate/Glycerol/L to 45% actate and Decrease Glucose, in Glucose can be
Lactate, Glucose decreased with SjvO2 below 42% seen with a decrease
Glutamat in SjvO2 to 40 to 45% e, Glycerol
(Unclear Interval)
Figaji et al Unclear Not PbtO2 LPR increased with low PbtO2 Not Specified High LPR is associated [21] Location Specified with low PbO2
Lactate, LPR, glycerol
(Unclear Interval)
Menzel et Unclear Varied PbtO2 Lactate decreased during increase in PaO2 and Not Specified Lactate decreases
al [57] Location therapies PbtO2 with increased PbtO2 directed Glucose, toward ICP Glucose displayed no relationship Lactate Group 1
(q30 min (n=12): FiO2 Measure) directed to
PaO2 of 100 to 150 mm Hg
Group 2 (n=12): Sequential increase in
FiO2 to 60% and then 100%
Menzel et Unclear Unclear PbtO2 During baseline measures there was no Not Specified Lactate may decrease
al [58] Location therapies; correlation between lactate and glucose with with increasing PbtO2
PbtO2 Glucose, N=14 with Lactate hyperoxia During hyperoxia Lactate decreased with a
therapy – corresponding increase in PbtO2. (q30 min sequential
Measure) increase in Glucose showed no clear trend with PbtO2
FiO2 up to druring hyperoxia. 100%
15 Nortje et al Unclear Standardize PbtO2 and O PET PbtO2: LPR decreased as PbtO2 increased during Not Specified LPR may decrease
[63] Location d Protocol hyperoxia. Not significant changes were note with increasing PbtO2 for lactate, pyruvate, glucose, glutamate and Glucose, Hyperoxia glycerol in isolation. Lactate, Therapy: Pyruvate, Unclear PET: 15O PET update focally was seen with Glutamat hyperoxia, but this did not correlate to LPR e, changes. Glycerol
(q20 min Measure) Purins et al Unclear ICP/CPP PbtO2 Glutamate increases significantly with PbtO2 Not Specified LPR, Glutamate and [72] Location directed below 5 mm Hg (p<0.05) Glycerol increase as
therapies; PbtO2 drops below 5
Glucose, variable Glycerol increases significantly with PbtO2 mm Hg. Glucose Lactate, treatments below 5 mm Hg (p<0.05) doesn’t respond to
Pyruvate, decrease PbtO2 levels.
Glutamat LPR increase with PbtO2 below 5 mm Hg e, (p<0.01) Glycerol No significant correlation between glucose and
(Hourly PbtO2 Measure)
Robertson Unclear Not PbtO2 and CBF High Glutamate/Aspartate levels were Not Specified High Glutamate levels et al [76] Location Specified (TCD) negatively correlated to diffuse brain injury, are associated with
PbtO2, and CBF (TCD) mortality Glutamat e
(q30 min Measure)
Sarrafzade Unclear Not PbtO2 As PbtO2 dropped to 10-15 mm Hg (for 5 min), Not Specified Increases in h et al [83] Location Specified glutamate increased (p=0.006) Glutamate, Lactate and LPR can be seen
Glucose, As PbtO2 drops below 10 mm Hg (5 min), with decreasing PbtO2 Lactate, Glutamate (p<0.001), Lactate (p=0.001), and Pyruvate, LPR (p=0.088) increased LPR, Glutamat e
(Hourly Measure) Sarrafzade Unclear Not PbtO2 Glucose dropped significantly prior to PbtO2 Not Specified Decreased glucose h et al [84] Location Specified decreasing to 10 mm Hg. may predict PbtO2 defined hypoxia.
Glucose, Glutamate displayed no relationship to PbtO2 Glutamate does not Lactate, seem to correlate. LPR, Glutamat e
(Hourly Measure)
Timofeev Mixed Standardize PbtO2 Strong negative correlation between LPR Not Specified LPR may correlate to
et al [85] Peri- d protocol; (p<0.001) and lactate (p<0.001) and PbtO2 PbtO2 Lesion individual and patients not Healthy all same Tissue
Glucose, Lactate, Pyruvate, LPR, Glycerol, Glutamat e
(Hourly Measure) Valdaka et Unclear Non- PbtO2 Lactate, Glutamate, LPR and potassium Not Specified Limited. Significant
al. [96] Location specific increase significantly as PbtO2 approaches zero. derrangements seen treatment during death. Glucose, Lactate, Glutamat e
(q30 min Measure)
Vilalta et al Healthy ICP/CPP PbtO2 During hyperoxia increases in PbtO2 (mean Not Specified Increased glucose [101] Tissue therapy; no increased from 26.9 mm Hg to 97.7 mm Hg) with decreases in very clear occur in concert with increases in glucose LPR/Lactate/Pyruvate Glucose, (p=0.037) and decreases in LPR (p=0.005), may be seen with
Lactate, Hyperoxia lactate (p<0.001) and pyruvate (p=0.002) increases in PbtO2 Pryuvate, Therapy: Glutamat obtain e baseline, then (Hourly increase
Measure) FiO2 to 100%
Autoregulation - Positive Association Studies
Asgari et al Unclear Unclear MOCAIP ICP Occasional LPR increases seen in circumstances Not Specified LPR may be increased [4] Location Therapy Waveform based of autoregulation dysfunction in situation with Autoregulation abnormal Lactate, Measurements autoregulation Pyruvate, LPR
(Unclear Interval) Asgari et al Unclear Not PMTM ICP Some association between LPR increase and Not Specified Increased LPR may [5] Location Specified Waveform Analysis vasoconstriction correlated to for vasoconstriction in Lactate, Vascoconstriction/V some cases Pyruvate, asodilatation LPR
(Unclear Interval)
Yokobori et Peri- Standard PRx There was a positive correlation between Not Specified LPR and Glucose al [105] Lesional ICP/CPP improvement in PRx and CMD glucose levels changes may directed correlate to PRx based Glucose, therapy There was a negative correlation between changes Glutamat improved PRx and LPR e, Glycerol, Lactate, Pyruvate, LPR
(Hourly Measure)
Imaging Based Positive Association Studies
Bouzat et al Healthy ICP/CPP CTP assessment of Low Glucose and elevated LPR were associated Not Specified Low Glucose and [11] Tissue Directed CBF during with a reduction in rCBF (p<0.05) elevate LPR correlated Therapy; no episodes of brain to a reduction in rCBF
Lactate, specifics hypoxemia (PbtO2 as per CTP Pyruvate, <20 mm Hg for 5 LPR, min) or “Abnormal” Glucose CMD measures (Glucose <1 mmol/L (Unclear and LPR >40) Interval) 15 Hutchinson Unclear Standard H2 O PET (with ROI Positive correlation between OEF and LPR Not Specified LPR and OEF seem to et al [39] Location Protocols; around probe (p=0.002) be positively no specifics location) correlated Glucose, Lactate, Pyruvate, Glutamat e
(q20 min Measure) Hutchinson Unclear Standard FDG PET (ROI Lactate and Pyruvate displayed a positive linear Not Specified Lactate, Pyruvate and et al [40] Location Protocol; no around probe correlation to CMRglc (p<0.0001) Glutamate displayed a further location) positive correlation to Glucose, details Weak positive correlation between CMRglc and CMRglc Lactate, Glutamate Pyruvate, Glutamat No relationship between CMRglc and LPR or e Glucose was seen
(q30 min Measure)
Reinert et Mixed Not Xe CT and ICP Negative correlation between potassium and Not Specified Potassium has a al [74] Peri- Specified CBF (p=0.019) negative correlation Lesion to Xe CT CBF and Positive correlation between mean potassium Healthy and ICP >30 mm Hg (p<0.0001) Tissue
Potassiu m, Lactate, Glutamat e
(q30 min Measure)
Sala et al Unclear Standard CTP at 24 and 48 CTP: Glycolytic Lactate elevations (normal Not Specified Hypoxic Lactate
[78] Location ICP/CPP hours post injury PbtO2) were associated with elevations are Protocol normal/supranormal perfusion. Hypoxic associated with global
Glucose, ICP lactate elevations (PbtO2 < 20 mm Hg for 5 min) oligemia Lactate, were associated with global oligemia. Pyruvate, Glutamat ICP: Glycolytic lactate elevations were not e associated with ICP elevations
(Hourly Measure)
15 Vespa et al Unclear Standard FDG PET and C O, LPR was negatively correlated to CMRO2 Not Specified LPR displays a 15 15 [97] Location ICP/CPP O O, H2 O PET (p<0.001) negative correlation
Directed (ROI around probe to CMRO2 Glucose, Therapy location) No other correlations detected Lactate, Pyruvate, Glutamat e, Glycerol
(Hourly Measure)
Vespa et al Healthy None FDG PET (ROI Mean daily CMD glucose = 0.05 to 3.2 mmol/L No Complications Glucose is positively [99] Tissue Mentioned around probe correlated to FDG PET location) and Xe CT CMD glucose value of 0.2 mmol/L (or lower) signal and Xe CT CBF Glucose, corresponded to an increase in FDG signal on Lactate PET
(Hourly CMD glucose positively correlated with Xe CT Measure) CBF measurements (p<0.001)
Zauner et Unclear Not Xe CT Elevations in glutamate corresponded Not Specified Elevations in al [109] Location Specified positively to reductions in CBF glutamate may correspond to Glutamat reductions in CBF as e assessed by Xe CT
(Unclear Interval)
Negative Association Studies Alessandri Unclear Not ICP No correlation between Sodium/Glutamate Not Specified Sodium and et al [3] Location Specified with ICP was identified Glutamate levels do not correlate with ICP Sodium, Glutamat e
(Unclear Interval) Chamoun Unclear Various ICP ICP/PbtO2/SjvO2 No correlation between glutamate and Not Specified Glutamate does not
et al [13] Location Therapies; MABP/ICP/PbtO2/SjvO2 correlate to
Some DC MABP/ICP/PbtO2/SjvO
Glutamat patients 2 e
(Hourly Measure)
Johnston et Healthy CPP CPP and PbtO2 No association between CMD measures and Not Specified CMD does not al [44] Brain Directed CPP correlate with CPP or
Therapy PbtO2 changes Glucose, with Unclear association between CMD measures
Lactate, augment to and PbtO2 Pyruvate, >70 mm Hg LPR, Glycerol
(Measure q30 min; unclear how correlated to outcome)
Nelson et al Bilateral Standard ICP/CPP No common patterns of CMD measures were Not Specified CMD measure do not [60] Location ICP/CPP seen in relation to ICP/CPP correlated to ICP/CPP (one in Therapy changes penumbra ; one in healthy)
Glucose, Lactate, Pyruvate, LPR, Glutamat e
(Hourly Collection )
Peerdeman Healthy ICP/CPP ICP/CPP No association between low CPP and increased Not Specified Glycerol elevations et al [70] Tissue Directed glycerol are not associated Therapy; with ICP/CPP changes Glucose, some No association between elevated ICP and Lactate, barbiturate glycerol Pyruvate, s and Glycerol hypothermi No association between elevated temperature a and glycerol (Unclear Interval)
Petzold et Mixed Not ICP Unclear relationship between Lactate, Pyruvate Not Specified Questionable al [71] Peri- Specified and LPR to ICP relationship between Lesion Lactate, Pyruvate and and LPR to ICP Healthy Tissue
Lactate, Pyruvate, LPR
(Hourly Measure) Sanchez- Unclear Local Long PRx (using 20 No correlation was seen between CMD Not Specified Glucose, Lactate, Porras et al Location Protocol; min averages of measures and Long PRx Pyruvate, Glutamate [81] Individual MAP and ICP data) do not correlate with Glucose, differences Long PRx defined Lactate, autoregulation Pyruvate, Glutamat e
(Hourly Measure)
Vespa et al Mixed Not CPP LPR changes occur independent of CPP Not Specified LPR changes occur [100] Peri- Specified changes. independent of CPP Lesion changes. and Healthy Tissue
Lactate, Pyruvate, LPR
(Hourly Measure; mean duration 120 hours) TBI = traumatic brain injury, GOS = Glasgow outcome scale, GOSE = Glasgow outcome scale extended, CMD = cerebral microdialysis, RCT = randomized control trial, ICP = intracranial pressure, CPP = cerebral perfusion pressure, NAA = N-acetyl acetate, CSF = cerebrospinal fluid, LPR = lactate:pyruvate ratio, CBF = cerebral blood flow, rCBF = regional cerebral blood flow, SjvO2 = jugular venous oxygen saturation, MABP = mean arterial blood pressure, PbtO2 = partial pressure of oxygen in brain tissue, Mx = autoregulation, PRx = pressure reactivity monitoring, TCD = transcranial Doppler, PET = positron emission tomography, FDG = fluorodeoxyglucose, OEF = oxygen extraction fraction, ROI = region of interest, CMRglc = cerebral metabolic rate of glucose consumption, CMRO2 = cerebral metabolic rate of oxygen consumption, Xe CT = xenon enhanced computed tomography, CTP = compute tomographic perfusion imaging, NIRS = near infrared spectroscopy, MMM = multi-modal monitoring, DC = decompressive craniectomy, mmol = milli-molar, mm Hg = millimeters of mercury, L = liter, umol = micromolar.