How to Complete the Transfer of Authorization Form (TAF)
We need to receive one signed TAF for each billing NPI (group or individual) that you bill your claims with. For example, if you are credentialed as an individual at Medicaid but are credentialed as a group with all other payers, then you will need to complete and return two TAF forms.
Also please note that this form must be completed by the authorized contact of the billing NPI.
Instructions for Completing the TAF Please print, sign, and return the TAF on the next page. The table below describes helpful tips for completing the TAF successfully.
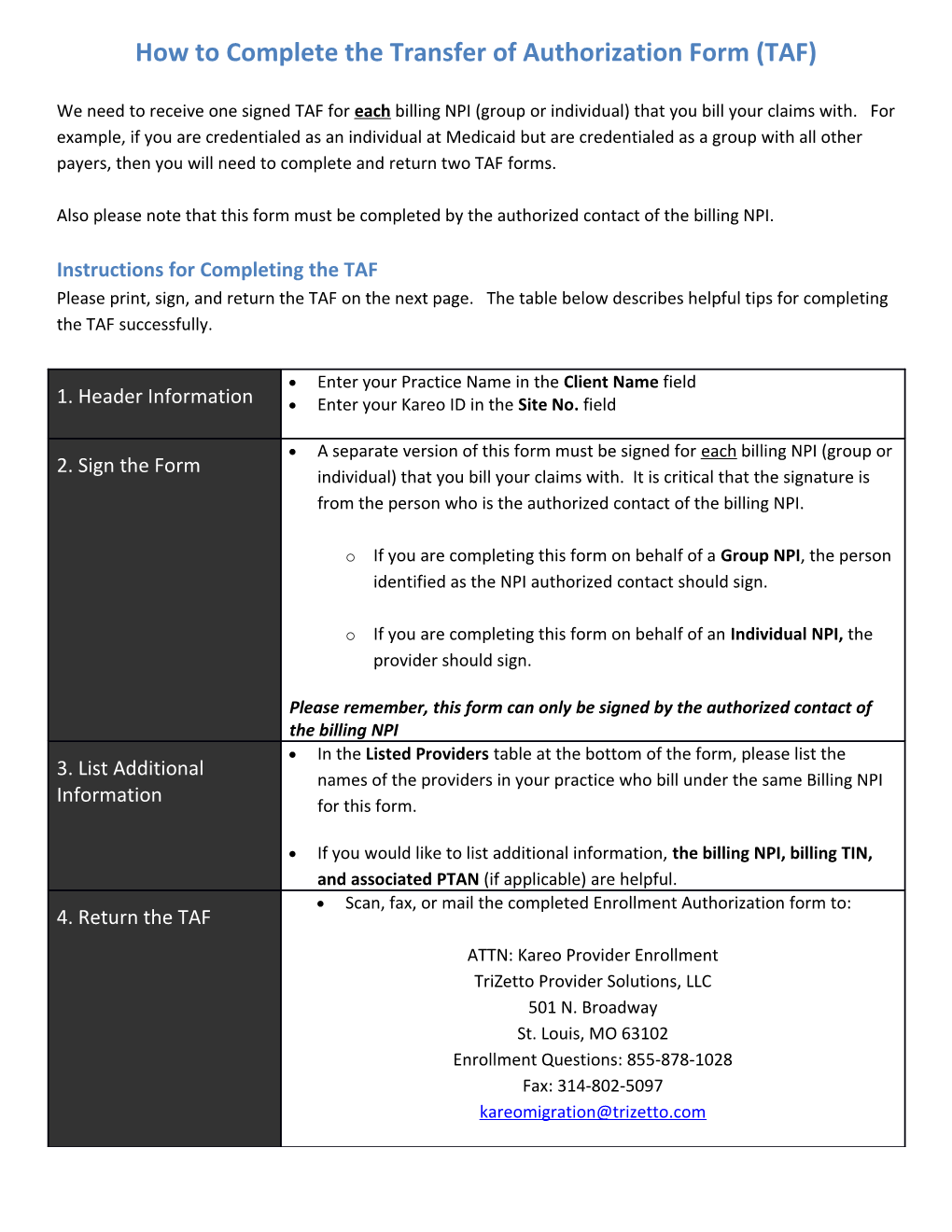
Enter your Practice Name in the Client Name field 1. Header Information Enter your Kareo ID in the Site No. field
A separate version of this form must be signed for each billing NPI (group or 2. Sign the Form individual) that you bill your claims with. It is critical that the signature is from the person who is the authorized contact of the billing NPI.
o If you are completing this form on behalf of a Group NPI, the person identified as the NPI authorized contact should sign.
o If you are completing this form on behalf of an Individual NPI, the provider should sign.
Please remember, this form can only be signed by the authorized contact of the billing NPI In the Listed Providers table at the bottom of the form, please list the 3. List Additional names of the providers in your practice who bill under the same Billing NPI Information for this form.
If you would like to list additional information, the billing NPI, billing TIN, and associated PTAN (if applicable) are helpful. Scan, fax, or mail the completed Enrollment Authorization form to: 4. Return the TAF ATTN: Kareo Provider Enrollment TriZetto Provider Solutions, LLC 501 N. Broadway St. Louis, MO 63102 Enrollment Questions: 855-878-1028 Fax: 314-802-5097 [email protected] ENROLLMENT AUTHORIZATION EDI Subscription Agreement
Client Name: Site No.:
CLIENT AUTHORIZATION By signing below, I certify that I have been appointed as the Client’s and the providers’ listed below (“Listed Providers”) authorized representative to whom the Client and Listed Providers have granted the legal authority to: (i) enroll the Listed Providers with any insurance plan, Medicare, and Medicaid (collectively, “Payers”) program, (ii) make changes and updates to the Listed Providers’ status in the Payers’ program; and (iii) commit the Listed Providers to abide by the applicable laws, regulations, and Payers’ instructions.
Furthermore, I authorize TriZetto Provider Solutions, LLC (“TriZetto”) to execute, print, copy, duplicate or otherwise affix my name to any Payer enrollment and registration forms (“Forms”) that may be required by such Payers to carry out the enumerated duties above.
I shall provide TriZetto with all necessary Listed Provider information (for example, NPI numbers, tax id numbers, etc.) for the limited purpose of TriZetto completing any Payer Forms. On behalf of Client and Listed Providers, I acknowledge that TriZetto will rely on the accuracy of the provided information.
Please sign below, keeping your signature within the box:
Printed Name: Title: Date:
LISTED PROVIDERS Please list the names of the Providers in Client’s organization below.
RETURN Scan, fax, or mail this Enrollment Authorization