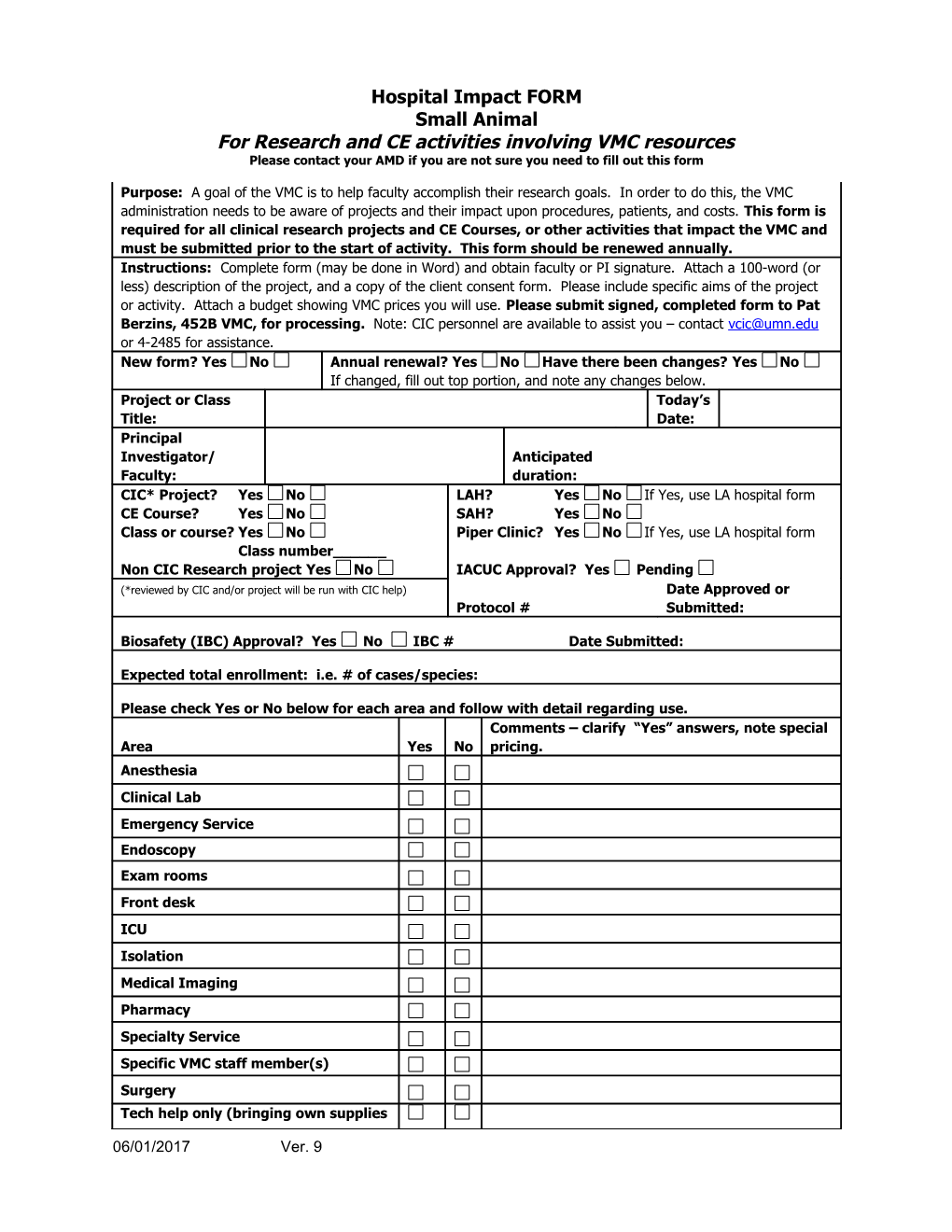
Hospital Impact FORM Small Animal For Research and CE activities involving VMC resources Please contact your AMD if you are not sure you need to fill out this form
Purpose: A goal of the VMC is to help faculty accomplish their research goals. In order to do this, the VMC administration needs to be aware of projects and their impact upon procedures, patients, and costs. This form is required for all clinical research projects and CE Courses, or other activities that impact the VMC and must be submitted prior to the start of activity. This form should be renewed annually. Instructions: Complete form (may be done in Word) and obtain faculty or PI signature. Attach a 100-word (or less) description of the project, and a copy of the client consent form. Please include specific aims of the project or activity. Attach a budget showing VMC prices you will use. Please submit signed, completed form to Pat Berzins, 452B VMC, for processing. Note: CIC personnel are available to assist you – contact [email protected] or 4-2485 for assistance. New form? Yes No Annual renewal? Yes No Have there been changes? Yes No If changed, fill out top portion, and note any changes below. Project or Class Today’s Title: Date: Principal Investigator/ Anticipated Faculty: duration: CIC* Project? Yes No LAH? Yes No If Yes, use LA hospital form CE Course? Yes No SAH? Yes No Class or course? Yes No Piper Clinic? Yes No If Yes, use LA hospital form Class number______Non CIC Research project Yes No IACUC Approval? Yes Pending (*reviewed by CIC and/or project will be run with CIC help) Date Approved or Protocol # Submitted:
Biosafety (IBC) Approval? Yes No IBC # Date Submitted:
Expected total enrollment: i.e. # of cases/species:
Please check Yes or No below for each area and follow with detail regarding use. Comments – clarify “Yes” answers, note special Area Yes No pricing. Anesthesia Clinical Lab Emergency Service Endoscopy Exam rooms Front desk ICU Isolation Medical Imaging Pharmacy Specialty Service Specific VMC staff member(s) Surgery Tech help only (bringing own supplies
06/01/2017 Ver. 9 etc) Specify where: Treatment room Wards
Central Supply (any special orders required, investigational drugs being shipped) Other Please list all chemicals, anesthetic gases, radiation, infectious agents and/or recombinant DNA that will be used in the study.
Describe any other budget considerations or agreements not listed above. For example: “Budget includes 6% increase for each new fiscal year per CIC” or “Study will entail a Saturday clinic, approved by Pat Berzins for Month, day, year”.
By signing below, I indicate that this information is complete to the best of my understanding. I understand that copies of clinical research documentation pertinent to this study may be sent to medical records for scanning and inclusion into DMS (Alchemy) for the official medical record. Studies that are confidential or externally sponsored are optional to be scanned in. NOTE: you may insert an electronic signature, or sign/scan and email completed form to Pat Berzins.
PI / Faculty Signature: Date Signed:
Hospital Administration: Date Signed: Submission checklist:
Yes N/A Did you fill in summary of project below?
Did you attach a copy of the Client Consent Form?
Did you receive pricing information? Please contact Pat Berzins or Kathy Stuebner.
Did you attach a budget?
Did you talk with Infection Control (Ashley Corcoran, [email protected]) re: chemicals, rDNA, etc?
Project summary:
06/01/2017 Ver. 9