CNS
Cranial Nerves
- Exit at base of the brain and pierce meninges to exit
- CNI (olfactory)- contact w/ external environment
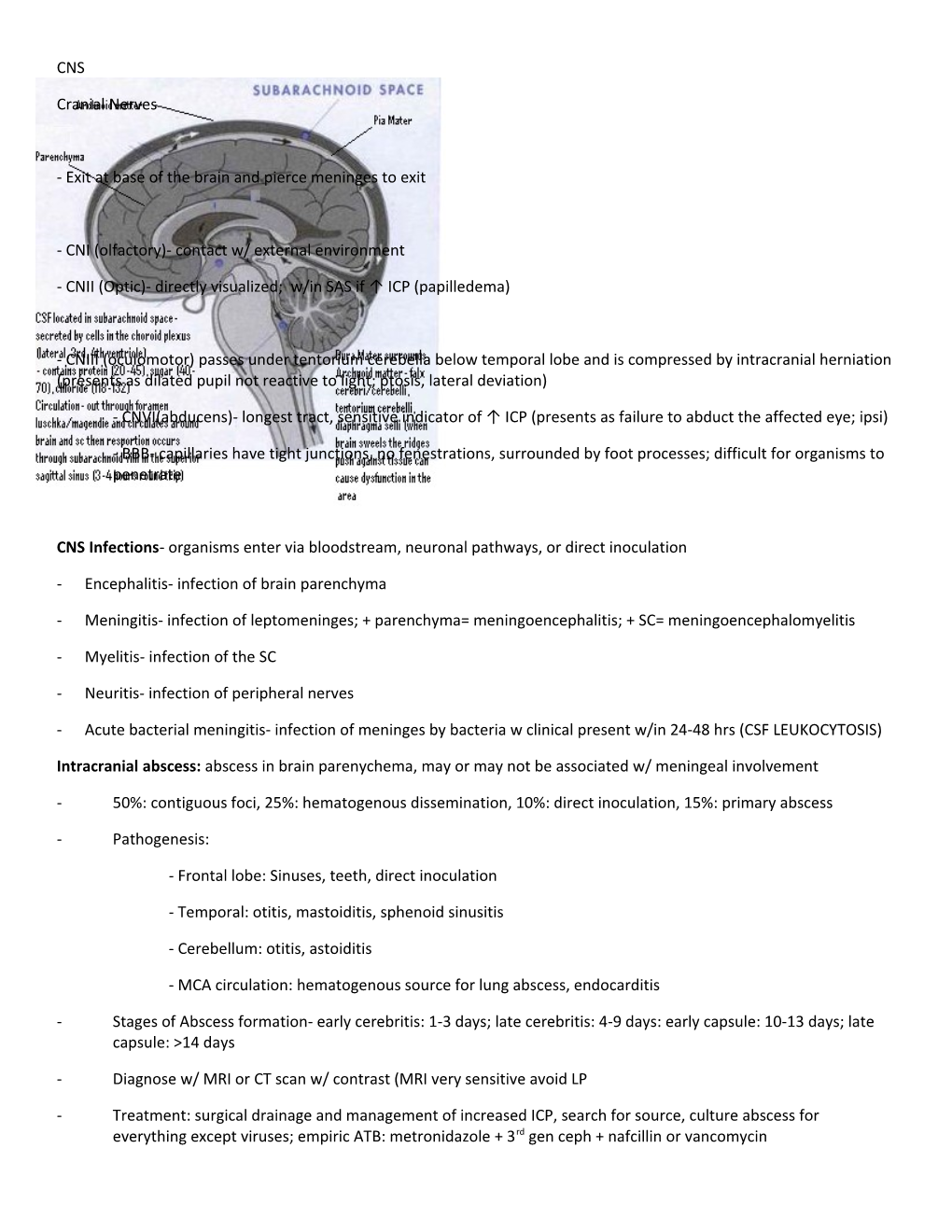
- CNII (Optic)- directly visualized; w/in SAS if ↑ ICP (papilledema)
- CNIII (oculomotor) passes under tentorium cerebella below temporal lobe and is compressed by intracranial herniation (presents as dilated pupil not reactive to light; ptosis, lateral deviation)
- CNVI(abducens)- longest tract, sensitive indicator of ↑ ICP (presents as failure to abduct the affected eye; ipsi)
- BBB- capillaries have tight junctions, no fenestrations, surrounded by foot processes; difficult for organisms to penetrate
CNS Infections- organisms enter via bloodstream, neuronal pathways, or direct inoculation
- Encephalitis- infection of brain parenchyma
- Meningitis- infection of leptomeninges; + parenchyma= meningoencephalitis; + SC= meningoencephalomyelitis
- Myelitis- infection of the SC
- Neuritis- infection of peripheral nerves
- Acute bacterial meningitis- infection of meninges by bacteria w clinical present w/in 24-48 hrs (CSF LEUKOCYTOSIS)
Intracranial abscess: abscess in brain parenychema, may or may not be associated w/ meningeal involvement
- 50%: contiguous foci, 25%: hematogenous dissemination, 10%: direct inoculation, 15%: primary abscess
- Pathogenesis:
- Frontal lobe: Sinuses, teeth, direct inoculation
- Temporal: otitis, mastoiditis, sphenoid sinusitis
- Cerebellum: otitis, astoiditis
- MCA circulation: hematogenous source for lung abscess, endocarditis
- Stages of Abscess formation- early cerebritis: 1-3 days; late cerebritis: 4-9 days: early capsule: 10-13 days; late capsule: >14 days
- Diagnose w/ MRI or CT scan w/ contrast (MRI very sensitive avoid LP
- Treatment: surgical drainage and management of increased ICP, search for source, culture abscess for everything except viruses; empiric ATB: metronidazole + 3rd gen ceph + nafcillin or vancomycin Encephalitis- inflammation of the brain, characterized by alteration in consciousness
- Many non-infectious disease: drug rxns, vasculitis
- Infectious is due to viral infection (bacteria, fungus, tubercular less common)
- Togavirus: EEE, WEE, VEE
- Flavi: SLE, West Nile
- Enteroviruses - Paramyxo- measles (rare)
- Rabies - Herpes: HSV 1, 2 and VZV (only treatable)
- Pathogenesis: Hematogenous (viral, rickettsia, bac, fungi, TB), Retrograde (rabies, VZV), olfactory nerves (virus)
- Diagnosis: EEG- slowing, MRI in HSV encephalitis shows temporal lobe involvement (PCR), LP w/ mild pleocytosis
- Treatment: acyclovir effective for HSV1, 2, VZV (always give, in case of false negative); supportive care
Subdural Empyema- pyogenic infection of space between dura and arachnoid
- Subdural space is crossed by small veins (emissary vessels); organisms reach subdural space this way or direct extension of osteomylitis of the skull
- Source: 50-80% frontal or ethmoid sinusitis; 10-20% otitis media/mastoiditis; 5% hematogenous dissemination
- Bacteriology: Polymicrobic infections are common: aerobic strep, staph, S. pneumo, H, inf, anaerobes, GNR
- 4:1 male to female; usually in 2nd or 3rd decade of life
- Diagnosis: MRI, very sensitive (diagnostic); CT scans will miss some; don’t do LP!
- Treatment: neurosurgery for burr holes or craniotomy; management of ↑ iCP (dexamethasone), culture of empyema fluid; simultaneous debridement of sinuses, mastoid, ear
- Treatment AB: min of 3 wks- cover anaerobes, GNR, GPC (metronidazole+cefriaxone+nafcillin or vancomycin
- Prognosis- 75% mortality if comatose, almost half develop seizures for life
Epidural abscess- located between bone and dura mater
- Intracranial epidural abscess- spills over into subdural space and forms subdural empyema too
- Treat/diagnosis same as subdural empyema
- Spinal epidural abscess- in spinal canal, epidural space-fat filled w/o emissary vessels, allows longitudinal spread
- Bacteria enter epidural space by direct extension (vertebral osteomyelitis) or hematogenous dissemin.
- Less often polymicrobial (S. aureus 60-90%, then streptococci, anaerobes, GNRs)
- Diagnosis: MRI, myelogram can visualize cord and look for compression, Blood cultures +, SED ↑
- Treatment: immediate surgical drainage; cover s. aureus, GNR and anaerobes pending cultures (Vanco+3rd gen ceph+metronidazole); prognosis if treated prior to paralysis is good
Abscess Intracranial Encephalitis Subdural Empyema Epidural Lesion Space occupying Rapidly expanding mass Focal deficit Yes (neuro) Yes (neuro) Yes (neuro) Yes (vertebral), spread/expand tenderness Fever <50% Yes Seizures Yes Yes Yes (later) Altered Mental Status Yes Yes Yes N/V Yes Yes Headache Yes Focal, later generalizes Ataxia Possible Visual field deficit Possible Personality Changes Yes ↓Consciousness Yes Hemiparesis Yes (later) Papilloedema <50% Radiculopathy Yes Motor/sensory Yes ↑ paralysis deficits Nuchal rigidity Yes Presentation of Acute Bacterial Meningitis
- Consider in patients w/ fever, neuologic symptoms, cerebral dysfunction
- Typical: HA, fever, lethargy, confusion, vomiting, stiff neck (varies); nuchal rigidity*
- Kernig’s (leg resistant to passive extension on inflammation)*
- brudzinski’s sign (flexion of neck causes pelvic thrust)*
- papilledema <1%
- *not good predictors
Pathogenesis of Meningitis- The outcome is Increased intracranial pressure
Nasopharyngeal colonization somehow get local invasion causing bactermia meningeal invasion replication SAS inflammation causes Increased BBB permeability (leads to vasogenic edema), cytotoxic edema, ↑ CSF outflow resistance (leads to hydrocephalus interstitial edema), and cerebral vasculitis and or infarction
Workup of Bacterial Meningitis
- CSF exam essential- Need to order WBC and DIFF, Glucose, Protein, Gram stain and Culture (special studies possible= hold last tube)
- Relative Contraindictation to LP (↑ ICP, platelet count <40,000, scoliosis, infected site over lumbar spine)
- To check ICP fast:
- Look at eyes, PERRL
- Look at optic disc to see if bulging (bad)
- Get them to follow finger w/ eyes (good= they can do it)
Treatment of Bacterial Meningitis
- If assessment for increased ICP is present you must obtain blood cultures, do empirical antimicrobial therapy CT scan of head if no mass lesion can do lumbar puncture
- If assessment for increased ICP is absent obtain blood cultures and perform lumbar puncture
- After LP- if consistent w/ bacterial meningitis then start treatment w/ dexamethasone and empirical antimicrobials by age if no positive gram stain and specific antimicrobials by agent if positive gram stain
- Cover commonly encountered pathogens: tx for 10-14 days
Cause Age Risk Vaccine Diagnosis Treatment
S. agalactiae 0-4 wks + bullet Amp or Pen G (gr. B) coccus E. coli 0-4 wks Neg rod 3rd gen ceph L. mono 0-4 wks, Neonates, pregnant women, elderly, + rod, Amp or Pen G >50 yr immune-compromise catalase + (trimeth-sulfa) H. influenza 4 wks- > 5 yo w/ sinusitis, otitis, epiglottis Type B type f Neg rod 3rd gen ceph 50 yrs pneumonia; Predisposing: DM, meningitis is ↑ ETOHism, asplenia, CSF leak, hypo- gammaglobenmia N. mening > 4 wks MAC complement defect (less fatal) A, C W135, Y; B Neg Amp or Pen G cause >50% infects diplococci S. pneumo > 4 wks #1 cause in 18-50 yo; w/ URTI, LRTI, Covers most + coccus Vanco+ 3rd gen endocarditis; Predisposing: see H. inf common serotypes ceph GNR > 50
Prime Bacteria Empirical treatment 0-4wks S. agalactiae, E. coli, L. monocytoes Amp+ 3rd gen ceph; or amp+AG 4wks-18 yrs H. inf, N. meningitides, S. pneumonia Vancomycin + 3rd gen ceph 18 yrs- 50 yrs H. inf, N. meningitides, S. pneumo Vancomycin + 3rd gen ceph 50 yrs L. monocytoes, N. meningitidies, S. pneumo, GNR Vancomycin + AG + 3rd gen ceph
Presentation of Acute Viral Meningitis
- Often aseptic meningitis
- Enteroviruses cause 80-85% of cases of viral meningitis; others include: arbovirus, herpes virus, HIV
Pathophysiology of Viral meningitis
- Muscosal colonization leads to viremia and virus crosses BBB (may travel along nerves)
- Virus enters SAS and spreads in the CSF inflammatory response specific for the virus (lymphocytes, Tcells)
Clinical Presentation of Viral meningitis
- Enterovirus in kids > 2 weeks old
- Sudden fever, frontal headache, photophobia, nuchal rigidity, and myalgias, d/v, anorexia, cough, sore throat
- Occurs more in summer months
- May be associated w/ enteroviral syndrome (classic rash, painful mouth vesicles)
- HSV 2 infection often associated w/ aseptic meningitis and signs of genital tract infections
- Initial episode of HIV may be associated w/ aseptic meningitis and AB may be negative
Treatment of Viral meningitis
- Enterovirus: consider use of gammaglobulin in extremely ill
- Herpes virus: acyclovir - HIV: consider triple drug therapy
Presentation of Chronic Meningitis
- Neurologic abnormalities or CSF abnormalities of > 4 wks duration
- Infections from: TB, nocardia, Cryptococcus, toxoplasmosis, syphilis, lyme disease, CMV
- Noninfectious causes: Behcet’s (autoimmune), carcinoma, vasculitis
- Often Insidious in onset: wax and wanes over weeks but w/ gradual neurologic decline
Diagnosis and Treatment of Chronic Meningitis
- Diagnostic workup is difficult: guide by history and PE plus lumbar punctures
- Treatment is guided by most likely initial diagnosis if the patient is critically ill or preferably by confirmation
CSF Findings
Bacterial Viral Fungal Tuberculosis WBC > 1000; PMNs <1000 (almost always <3,000); < 500; mononuclear < 1000; mononuclear lymphs Glucose < 45 or < 2/3 Normal Normal or low < 45 (abn. w/ AB) serum glucose (except HSV, LCM, mumps, EEE) Protein > 80 Mildly ↑ Protein >60 >>100 Grain stain + 80% of time negative negative AFB smear Culture + 80% of time Viral Culture difficult; PCR- HSV Special smears/culture Culture +