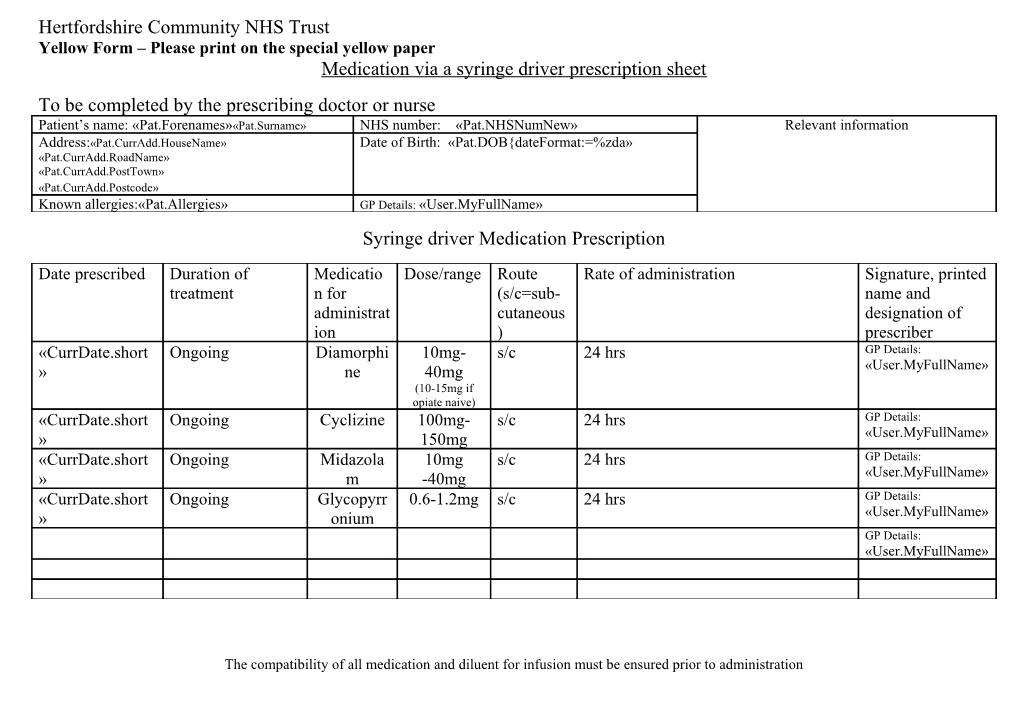
Hertfordshire Community NHS Trust Yellow Form – Please print on the special yellow paper Medication via a syringe driver prescription sheet To be completed by the prescribing doctor or nurse Patient’s name: «Pat.Forenames»«Pat.Surname» NHS number: «Pat.NHSNumNew» Relevant information Address:«Pat.CurrAdd.HouseName» Date of Birth: «Pat.DOB{dateFormat:=%zda» «Pat.CurrAdd.RoadName» «Pat.CurrAdd.PostTown» «Pat.CurrAdd.Postcode» Known allergies:«Pat.Allergies» GP Details: «User.MyFullName» Syringe driver Medication Prescription
Date prescribed Duration of Medicatio Dose/range Route Rate of administration Signature, printed treatment n for (s/c=sub- name and administrat cutaneous designation of ion ) prescriber «CurrDate.short Ongoing Diamorphi 10mg- s/c 24 hrs GP Details: » ne 40mg «User.MyFullName» (10-15mg if opiate naive) «CurrDate.short Ongoing Cyclizine 100mg- s/c 24 hrs GP Details: » 150mg «User.MyFullName» «CurrDate.short Ongoing Midazola 10mg s/c 24 hrs GP Details: » m -40mg «User.MyFullName» «CurrDate.short Ongoing Glycopyrr 0.6-1.2mg s/c 24 hrs GP Details: » onium «User.MyFullName» GP Details: «User.MyFullName»
The compatibility of all medication and diluent for infusion must be ensured prior to administration Palliative care medication to be prescribed in line with the Mount Vernon Palliative Adult Network Guidelines (3rd edition 2011) Prescription sheet number ………