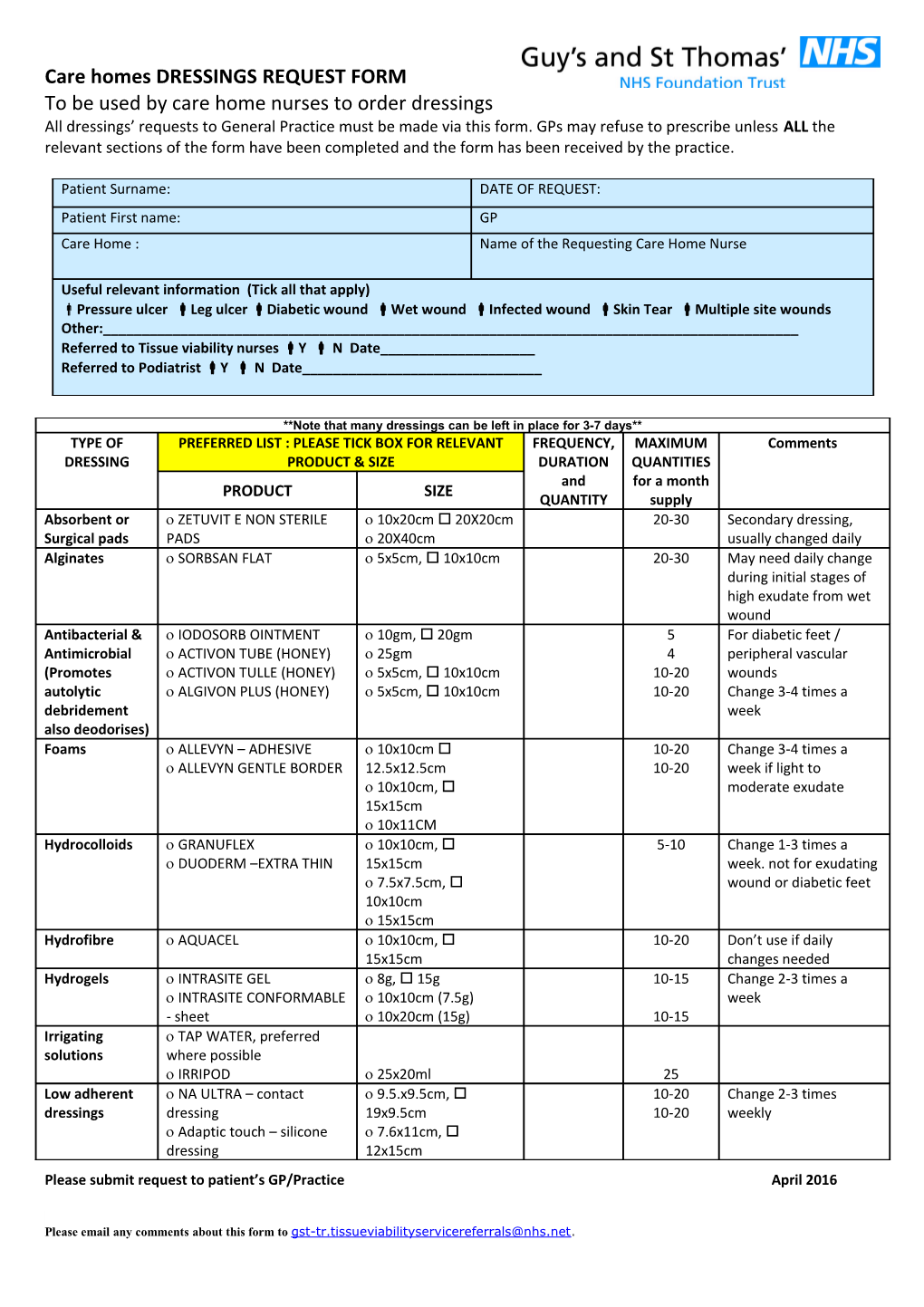
Care homes DRESSINGS REQUEST FORM To be used by care home nurses to order dressings All dressings’ requests to General Practice must be made via this form. GPs may refuse to prescribe unless ALL the relevant sections of the form have been completed and the form has been received by the practice.
Patient Surname: DATE OF REQUEST: Patient First name: GP Care Home : Name of the Requesting Care Home Nurse
Useful relevant information (Tick all that apply) Pressure ulcer Leg ulcer Diabetic wound Wet wound Infected wound Skin Tear Multiple site wounds Other:______Referred to Tissue viability nurses Y N Date______Referred to Podiatrist Y N Date______
**Note that many dressings can be left in place for 3-7 days** TYPE OF PREFERRED LIST : PLEASE TICK BOX FOR RELEVANT FREQUENCY, MAXIMUM Comments DRESSING PRODUCT & SIZE DURATION QUANTITIES and for a month PRODUCT SIZE QUANTITY supply Absorbent or ZETUVIT E NON STERILE 10x20cm 20X20cm 20-30 Secondary dressing, Surgical pads PADS 20X40cm usually changed daily Alginates SORBSAN FLAT 5x5cm, 10x10cm 20-30 May need daily change during initial stages of high exudate from wet wound Antibacterial & IODOSORB OINTMENT 10gm, 20gm 5 For diabetic feet / Antimicrobial ACTIVON TUBE (HONEY) 25gm 4 peripheral vascular (Promotes ACTIVON TULLE (HONEY) 5x5cm, 10x10cm 10-20 wounds autolytic ALGIVON PLUS (HONEY) 5x5cm, 10x10cm 10-20 Change 3-4 times a debridement week also deodorises) Foams ALLEVYN – ADHESIVE 10x10cm 10-20 Change 3-4 times a ALLEVYN GENTLE BORDER 12.5x12.5cm 10-20 week if light to 10x10cm, moderate exudate 15x15cm 10x11CM Hydrocolloids GRANUFLEX 10x10cm, 5-10 Change 1-3 times a DUODERM –EXTRA THIN 15x15cm week. not for exudating 7.5x7.5cm, wound or diabetic feet 10x10cm 15x15cm Hydrofibre AQUACEL 10x10cm, 10-20 Don’t use if daily 15x15cm changes needed Hydrogels INTRASITE GEL 8g, 15g 10-15 Change 2-3 times a INTRASITE CONFORMABLE 10x10cm (7.5g) week - sheet 10x20cm (15g) 10-15 Irrigating TAP WATER, preferred solutions where possible IRRIPOD 25x20ml 25 Low adherent NA ULTRA – contact 9.5.x9.5cm, 10-20 Change 2-3 times dressings dressing 19x9.5cm 10-20 weekly Adaptic touch – silicone 7.6x11cm, dressing 12x15cm Please submit request to patient’s GP/Practice April 2016
Please email any comments about this form to [email protected]. Care homes DRESSINGS REQUEST FORM To be used by care home nurses to order dressings All dressings’ requests to General Practice must be made via this form. GPs may refuse to prescribe unless ALL the relevant sections of the form have been completed and the form has been received by the practice.
**Note that many dressings can be left in place for 3-7 days** TYPE OF PREFERRED LIST : PLEASE TICK BOX FOR RELEVANT FREQUENCY, MAXIMUM Comments DRESSING PRODUCT & SIZE DURATION QUANTITIES PRODUCT SIZE and for a month Moisturisers ZERODERM OINTMENT 500g QUANTITY supply1 HYDROMOL OINTMENT 500g 1 HYDROMOL BATH AND 500ml SHOWER EMOLLIENT Retention & K-BAND (Retention) 10cmx4m 10-15 Change 2-3 times a Support K-SOFT (Wadding) 10cmx4m 10-15 week bandages K-LITE (Crepe for support) 10cmx4m 10-15 To pad bony parts Crepe is to provide support & help reduce ACTIFAST large limb-BLUE 7.5cmx5m 1 odema. Apply from toe ACTIFAST extra- YELLOW 10.75cmx5m 1 to knee Silver dressings SILVERCEL Non-Addherent 11x11cm, Change 2 times a week. (only if there 10x20cm 5 maximum 2 weeks are localised supply clinical signs of infection) Sterile dressings NURSE-IT S M L XL 10-30 packs WOUNDCARE STERILE S M L 10-30 PACK Surgical SCANPOR TAPE 2.5cm, 5cm 4 adhesive tapes HYPAFIX 5cmx10m, 2-3 Hypafix to secure 10cmx10m Zetuvit pads Vapour TEGADERM 12cm, 15x20cm 10-15 permeable dressings NON-PREFERRED LIST REQUESTS – EXCEPTIONAL REASONS ONLY PRODUCT NAME PRODUCT SIZE FREQUENCY , REASON FOR NON-PREFERRED LIST REQUEST. DURATION and (MUST BE COMPLETED OR THE PRODUCT QUANTITY (e.g. 2 CANNOT BE SUPPLIED) bd, 3/7, x10)
SUPPLY OF DRESSINGS TO THE PATIENT ( Confirm that this is accordance with the patient’s wishes) Tick the most appropriate box Patient or representative collecting prescription from GP practice
Please submit request to patient’s GP/Practice April 2016
Please email any comments about this form to [email protected]. Care homes DRESSINGS REQUEST FORM To be used by care home nurses to order dressings All dressings’ requests to General Practice must be made via this form. GPs may refuse to prescribe unless ALL the relevant sections of the form have been completed and the form has been received by the practice.
**Note that many dressings can be left in place for 3-7 days** TYPE OF PREFERRED LIST : PLEASE TICK BOX FOR RELEVANT FREQUENCY, MAXIMUM Comments DRESSING PRODUCT & SIZE DURATION QUANTITIES PRODUCT SIZE and for a month Prescription to be sent to ______PHARMACY.QUANTITY Pharmacysupply delivers (Tick if known)
Please submit request to patient’s GP/Practice April 2016
Please email any comments about this form to [email protected].