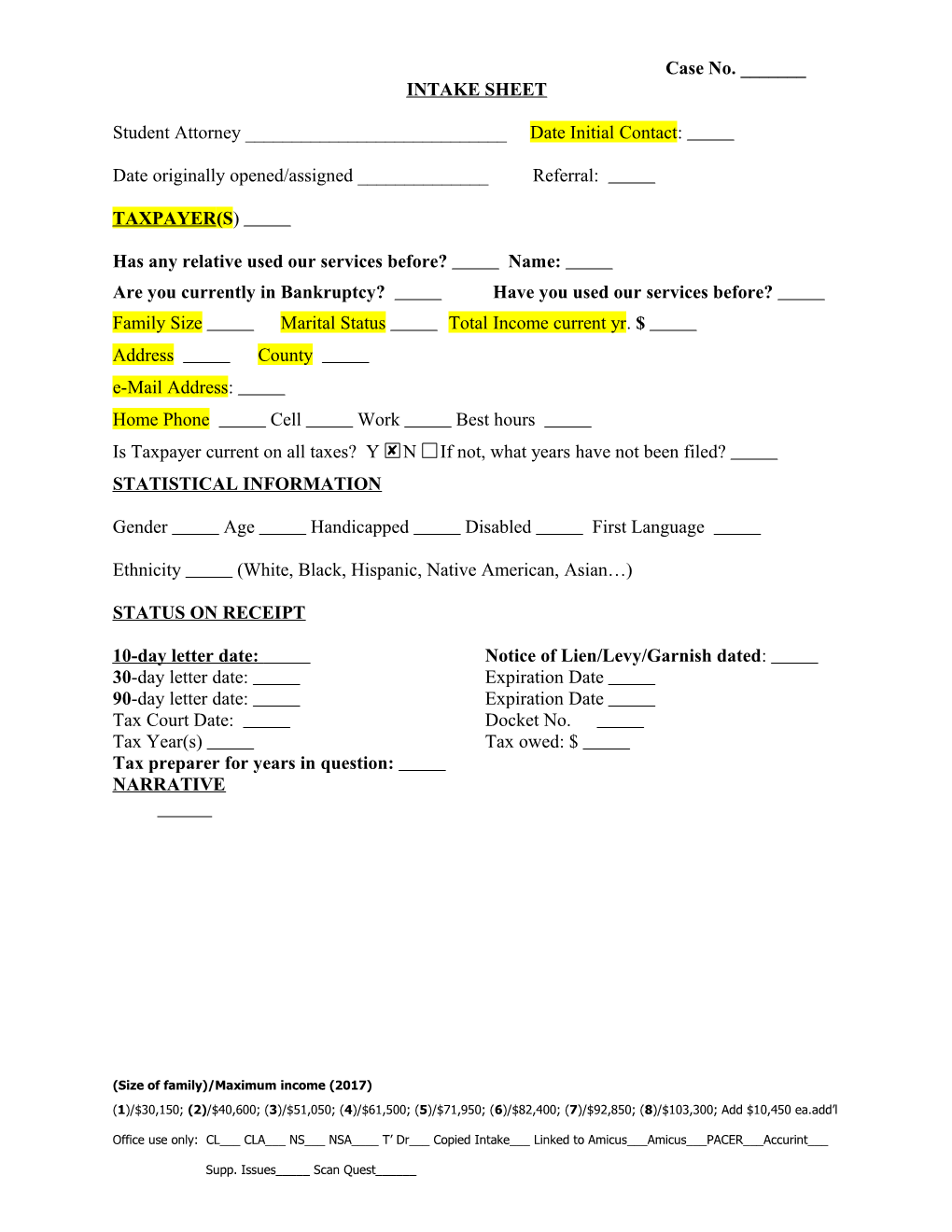
Case No. ______INTAKE SHEET
Student Attorney ______Date Initial Contact:
Date originally opened/assigned ______Referral:
TAXPAYER(S)
Has any relative used our services before? Name: Are you currently in Bankruptcy? Have you used our services before? Family Size Marital Status Total Income current yr. $ Address County e-Mail Address: Home Phone Cell Work Best hours Is Taxpayer current on all taxes? Y N If not, what years have not been filed? STATISTICAL INFORMATION
Gender Age Handicapped Disabled First Language
Ethnicity (White, Black, Hispanic, Native American, Asian…)
STATUS ON RECEIPT
10- day letter date: Notice of Lien/Levy/Garnish dated: 30-day letter date: Expiration Date 90-day letter date: Expiration Date Tax Court Date: Docket No. Tax Year(s) Tax owed: $ Tax preparer for years in question: NARRATIVE
(Size of family)/Maximum income (2017) (1)/$30,150; (2)/$40,600; (3)/$51,050; (4)/$61,500; (5)/$71,950; (6)/$82,400; (7)/$92,850; (8)/$103,300; Add $10,450 ea.add’l
Office use only: CL___ CLA___ NS___ NSA____ T’ Dr___ Copied Intake___ Linked to Amicus___Amicus___PACER___Accurint___
Supp. Issues_____ Scan Quest______Case No. ______Step 1: Complete Basic Intake & Route to Conflicts Referral: Date:
Clinic: Investor Advocacy HeLP Tax Potential Client Name: Address: Phone Number: Home Cell Work E-mail Address (personal only): Other Potential Clients: Potentially Adverse Parties: Brief Description of Matter: (not needed for Tax Clinic)
ROUTE TO CONFLICTS: Date: By:
Step 2: Complete Conflicts Check
Conflicts Check:
Date Completed: ______By: ______
Names Searched No Match Match
IF MATCH FOUND, CONTACT MARIANA CHRISTINA PANNELL
(Size of family)/Maximum income (2017) (1)/$30,150; (2)/$40,600; (3)/$51,050; (4)/$61,500; (5)/$71,950; (6)/$82,400; (7)/$92,850; (8)/$103,300; Add $10,450 ea.add’l
Office use only: CL___ CLA___ NS___ NSA____ T’ Dr___ Copied Intake___ Linked to Amicus___Amicus___PACER___Accurint___
Supp. Issues_____ Scan Quest______Case No. ______
Name:
Step 3: Make Representation Decision and Route to Conflicts
Representation Determination:
Clinic accepted representation: Yes No (circle one).
If no: Date non-engagement (declination) letter sent: ______
If yes: Date signed engagement letter received from client: ______
The parties listed on the initial contact check are correct: Yes No (circle one) If no, please note any changes here:
Representation decision entered into Clio by: ______Date: ______
Step 4: Close File and Route to Conflicts
Accepted matter concludes
Representation concluded on: ______Disengagement letter sent: Yes___ No___
Entered into Conflicts database by: ______Date: ______
(Size of family)/Maximum income (2017) (1)/$30,150; (2)/$40,600; (3)/$51,050; (4)/$61,500; (5)/$71,950; (6)/$82,400; (7)/$92,850; (8)/$103,300; Add $10,450 ea.add’l
Office use only: CL___ CLA___ NS___ NSA____ T’ Dr___ Copied Intake___ Linked to Amicus___Amicus___PACER___Accurint___
Supp. Issues_____ Scan Quest______