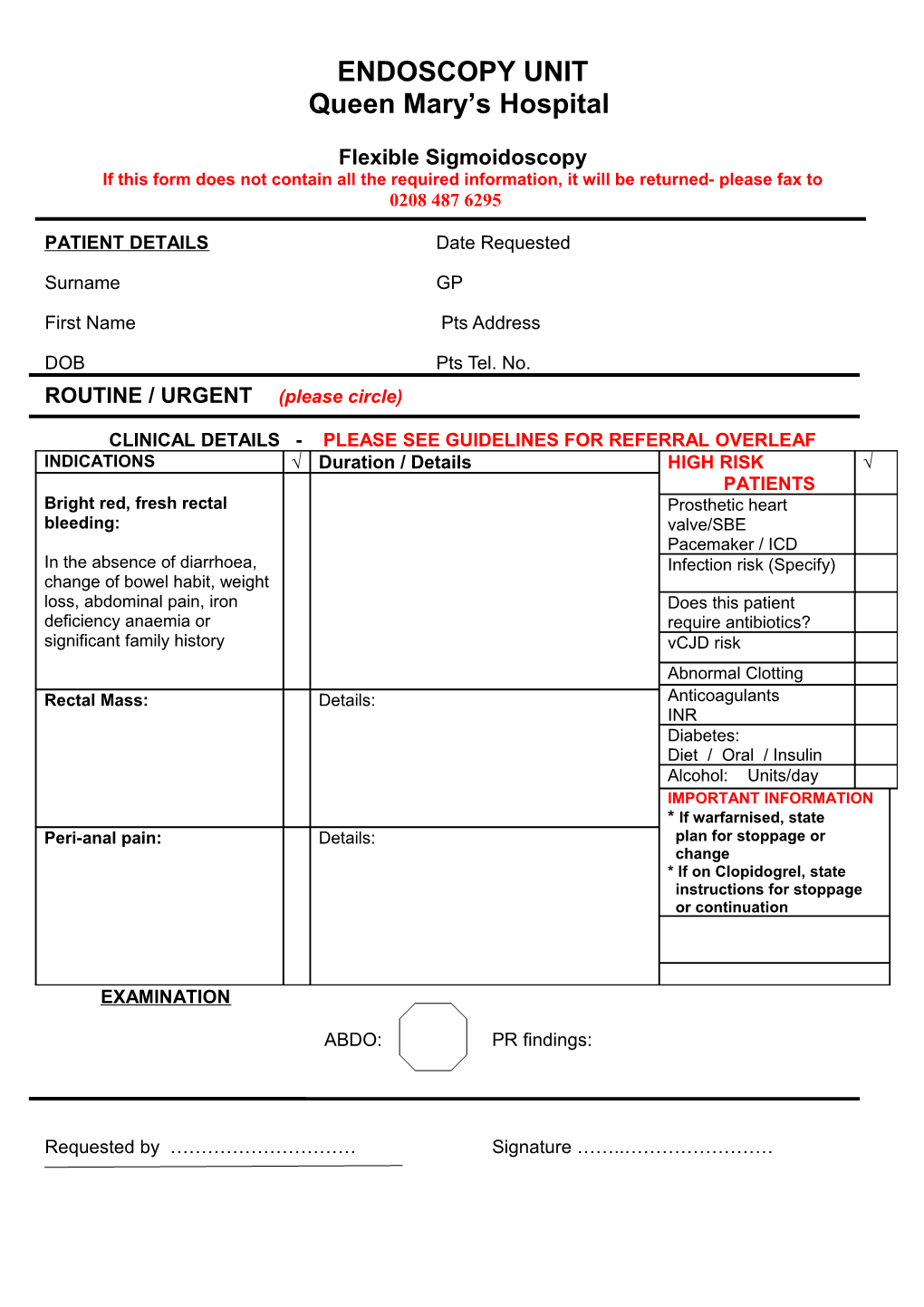
ENDOSCOPY UNIT Queen Mary’s Hospital
Flexible Sigmoidoscopy If this form does not contain all the required information, it will be returned- please fax to 0208 487 6295
PATIENT DETAILS Date Requested
Surname GP
First Name Pts Address
DOB Pts Tel. No. ROUTINE / URGENT (please circle)
CLINICAL DETAILS - PLEASE SEE GUIDELINES FOR REFERRAL OVERLEAF INDICATIONS Duration / Details HIGH RISK PATIENTS Bright red, fresh rectal Prosthetic heart bleeding: valve/SBE Pacemaker / ICD In the absence of diarrhoea, Infection risk (Specify) change of bowel habit, weight loss, abdominal pain, iron Does this patient deficiency anaemia or require antibiotics? significant family history vCJD risk Abnormal Clotting Rectal Mass: Details: Anticoagulants INR Diabetes: Diet / Oral / Insulin Alcohol: Units/day IMPORTANT INFORMATION * If warfarnised, state Peri-anal pain: Details: plan for stoppage or change * If on Clopidogrel, state instructions for stoppage or continuation
EXAMINATION
ABDO: PR findings:
Requested by ………………………… Signature ……..……………………