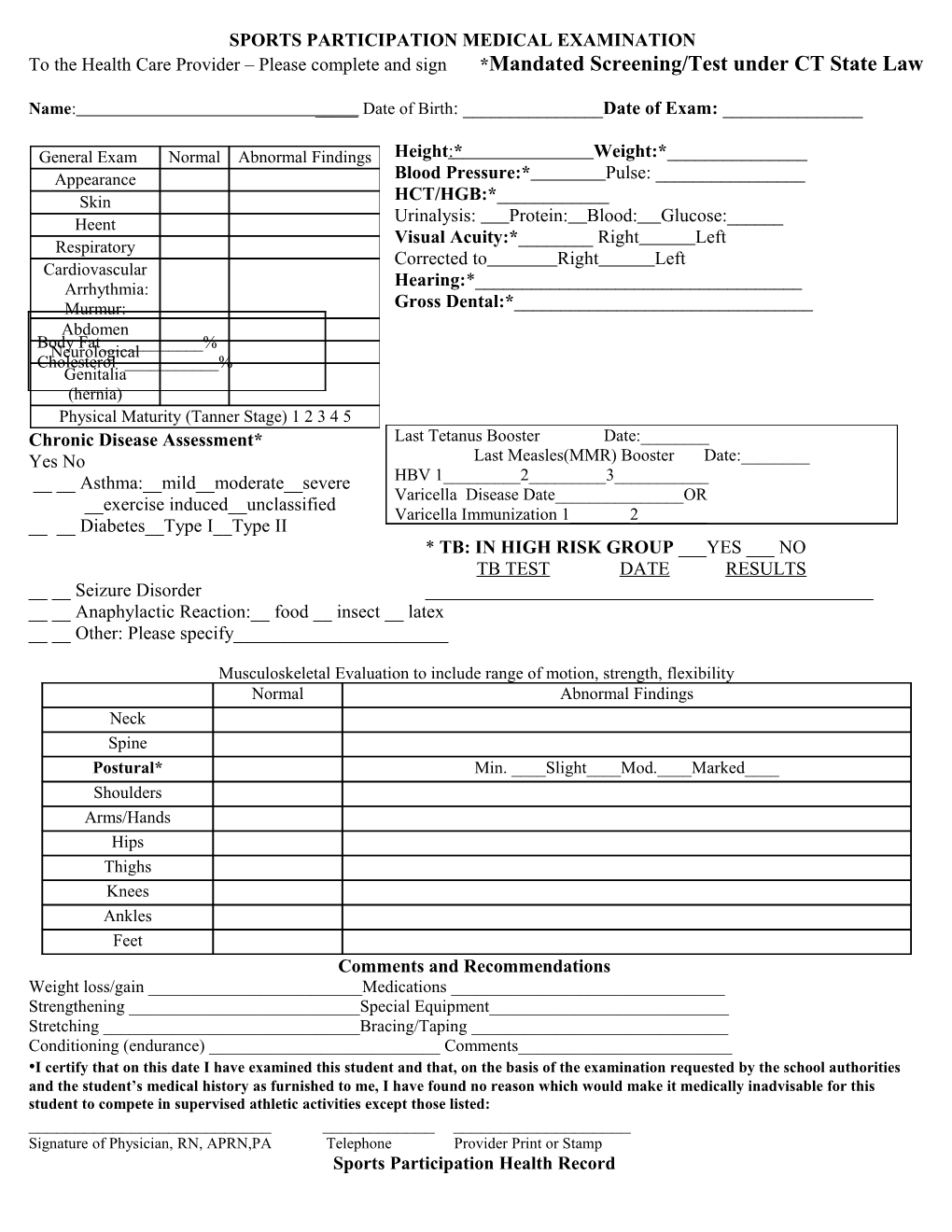
SPORTS PARTICIPATION MEDICAL EXAMINATION To the Health Care Provider – Please complete and sign *Mandated Screening/Test under CT State Law
Name: _____ Date of Birth: ______Date of Exam: ______
General Exam Normal Abnormal Findings Height : * Weight:*______Appearance Blood Pressure:* Pulse: ______Skin HCT/HGB:*______Heent Urinalysis: Protein: Blood: Glucose:______Visual Acuity:*______Right Left Respiratory Corrected to Right Left Cardiovascular Arrhythmia: Hearing:*______Murmur: Gross Dental:*______Abdomen Body Fat______% Neurological Cholesterol ______% Genitalia (hernia) Physical Maturity (Tanner Stage) 1 2 3 4 5 Chronic Disease Assessment* Last Tetanus Booster Date:______Yes No Last Measles(MMR) Booster Date:______Asthma:__mild__moderate__severe HBV 1______2______3______Varicella Disease Date______OR __exercise induced__unclassified Varicella Immunization 1______2______Diabetes__Type I__Type II * TB: IN HIGH RISK GROUP ___YES ___ NO TB TEST DATE RESULTS __ __ Seizure Disorder ______Anaphylactic Reaction:__ food __ insect __ latex __ __ Other: Please specify______
Musculoskeletal Evaluation to include range of motion, strength, flexibility Normal Abnormal Findings Neck Spine Postural* Min. ____Slight____Mod.____Marked____ Shoulders Arms/Hands Hips Thighs Knees Ankles Feet Comments and Recommendations Weight loss/gain ______Medications ______Strengthening ______Special Equipment______Stretching ______Bracing/Taping ______Conditioning (endurance) ______Comments______•I certify that on this date I have examined this student and that, on the basis of the examination requested by the school authorities and the student’s medical history as furnished to me, I have found no reason which would make it medically inadvisable for this student to compete in supervised athletic activities except those listed: ______Signature of Physician, RN, APRN,PA Telephone Provider Print or Stamp Sports Participation Health Record This evaluation is to determine readiness for sports participation. This must be completed by a parent and student before being brought to the Doctor’s office.
Name:______Age:_____Sex:_____School______Address:______Phone:______Grade:______Sports being played (1)______(2)______(3)______Medical History (To be completed by student and parent/guardian) 1.Do you have any allergies?(Drugs, Food, Insect Stings, etc.) ______yes; List______No 2. Are you currently taking any drugs or medications including steroids or protein supplements(Daily or occasionally) ______yes; List______No 3. Are you presently being treated for any condition by a physician or other health care professional? ______yes; Explain______No 4. Have you ever been advised by a doctor not to participate in any sport? ______yes; Explain______No 5. Do you have any chronic conditions, disorders or diseases? Check those applicable or….______No ______Asthma ____Bleeding Disorders ____Diabetes ___Epilepsy(Seizures) ______Hepatitis(liver disease) ____Hypertension(High Blood Pressure) ____Sickle Cell Anemia ___Other______Mononucleosis-Yr ______Kawasaki Disease ____Disability (describe)______
Please Check where applicable if you have or have had any of the following: Yes No Yes No Head injury, concussion, or been unconscious ______Eye injury or retinal detachment ______If yes, how many times______Blurred vision or vision in one eye only ______Headaches more than once a week ______Wear glasses or contact lenses ______Lack of feeling or numbness in any part of the body______Hearing loss or impairment in one or both ears Heat exhaustion or heat stroke ______Tubes in ears or perforated ear drum ______Difficulty running ½ mile without stopping ______False teeth, caps or braces ______Chest pain, dizziness or passing out during exercise ______Nose bleeds for no reason ______Coughing, wheezing or gasping for breath Bruising easily or taking a long time to stop bleeding with exercise or cold weather ______when cut ______Smoke cigarettes or chew tobacco ______Diarrhea more than once a week ______Heart problem, murmur or arrhythmia ______Black or bloody bowel movements (stools) ______Family member with a heart attack under age 50 ______Kidney disease or dark, brown or bloody urine ______Loss or gain of more than 10 lbs. in last year ______Less than two kidneys or in males, two testicles ______Special diet for medical reasons ______Lump(s) in arm pit or groin ______For female participants Rash or skin problem ______Absent or irregular monthly periods ______Neck, spine or low back injury or pain ______Disabling cramps with your menstrual periods ______Have you ever been hospitalized for medical or surgical reasons? __ __ If yes, provide the following information: Reason Year Hospital ______
Please carefully list below any injury (nerve, muscle, bone or joint) that you have had which did not allow you to participate in regular activity for a week or more. Injured Area Year Side Type Resolved ( knee, Hamstring, Neck, Shin, etc.) ______(R/L) (Fracture, Sprain, Swelling, Pinched Nerve, etc. Yes No ______Student and Parent or Guardian: We hearby state that we have reviewed this medical history and found the information supplied above to be correct to the best of our knowledge.
______Student Signature Date Parent/Guardian Signature Date SHM Vol. I Sec. 6 7/06 Physical Exam Requirements for Interscholastic Sports Participation To participate in interscholastic sports at the Varsity, JV or Freshman level, students are required to have a physical exam on record in the nurse's office by their health care provider (physician, physician's assistant, APRN or RN.)
This exam must have been done within thirteen (13) months prior to the start of tryouts, practices, or play in the particular sport in which the student plans to participate. If this physical expires during the sport season, a new physical must be submitted to the nurse in order for the student to continue participating in that sport. This physical must be on record PRIOR to try-outs; there are no exceptions.
All health assessments must be complete. Both sides must be completed (one side by parent and one side by the health care provider) and every item marked with an asterisk * must be filled in. Per our policy, any health assessment that has missing mandated information will be considered incomplete and will be returned to you for completion. This will delay a student’s participation in sport as students will not be allowed to try out, practice or play until the form is completed.
Points to Remember:
Due to the large number of students who participate in sports, it is often difficult to get an appointment with your health care provider on a last minute basis. Parents whose children plan to participate in a sport are urged to make an appointment with their health care provider well in advance of the intended sports season. We recommend you keep a copy of your child’s physical for your records at home.
Physicals are to be submitted to the nurse’s office, not the coach . Coaches can not clear a student medically to participate in sports. Please hand in your physical as soon as it is completed. Do not wait for the sports season to begin.
Deadline for handing in physicals for the fall sport season is: Friday, August 13, 2010 for Football Friday, August 20, 2010 for all other sports
The Health Office will be glad to help you clarify any matter relating to sports physicals. Please call 255-7204 for assistance.