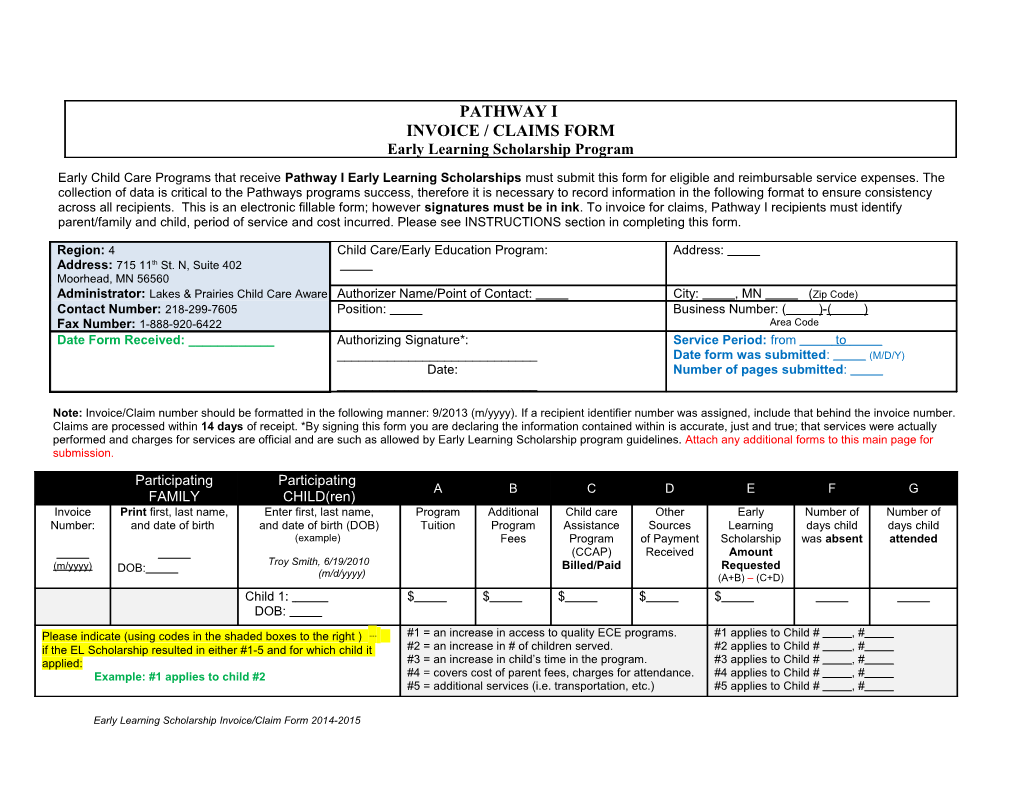
PATHWAY I INVOICE / CLAIMS FORM Early Learning Scholarship Program
Early Child Care Programs that receive Pathway I Early Learning Scholarships must submit this form for eligible and reimbursable service expenses. The collection of data is critical to the Pathways programs success, therefore it is necessary to record information in the following format to ensure consistency across all recipients. This is an electronic fillable form; however signatures must be in ink. To invoice for claims, Pathway I recipients must identify parent/family and child, period of service and cost incurred. Please see INSTRUCTIONS section in completing this form.
Region: 4 Child Care/Early Education Program: Address: Address: 715 11th St. N, Suite 402 Moorhead, MN 56560 Administrator: Lakes & Prairies Child Care Aware Authorizer Name/Point of Contact: City: , MN (Zip Code) Contact Number: 218-299-7605 Position: Business Number: ( )- ( ) Fax Number: 1-888-920-6422 Area Code Date Form Received: ______Authorizing Signature*: Service Period: from to ______Date form was submitted: (M/D/Y) Date: Number of pages submitted: ______
Note: Invoice/Claim number should be formatted in the following manner: 9/2013 (m/yyyy). If a recipient identifier number was assigned, include that behind the invoice number. Claims are processed within 14 days of receipt. *By signing this form you are declaring the information contained within is accurate, just and true; that services were actually performed and charges for services are official and are such as allowed by Early Learning Scholarship program guidelines. Attach any additional forms to this main page for submission.
Participating Participating A B C D E F G FAMILY CHILD(ren) Invoice Print first, last name, Enter first, last name, Program Additional Child care Other Early Number of Number of Number: and date of birth and date of birth (DOB) Tuition Program Assistance Sources Learning days child days child (example) Fees Program of Payment Scholarship was absent attended (CCAP) Received Amount Troy Smith, 6/19/2010 (m/yyyy) DOB: Billed/Paid Requested (m/d/yyyy) (A+B) – (C+D) Child 1: $ $ $ $ $ DOB: Please indicate (using codes in the shaded boxes to the right ) ⇢ #1 = an increase in access to quality ECE programs. #1 applies to Child # , # if the EL Scholarship resulted in either #1-5 and for which child it #2 = an increase in # of children served. #2 applies to Child # , # applied: #3 = an increase in child’s time in the program. #3 applies to Child # , # Example: #1 applies to child #2 #4 = covers cost of parent fees, charges for attendance. #4 applies to Child # , # #5 = additional services (i.e. transportation, etc.) #5 applies to Child # , #
Early Learning Scholarship Invoice/Claim Form 2014-2015 INSTRUCTIONS FOR COMPLETING THE EARLY LEARNING SCHOLARSHIPS INVOICE/ CLAIMS FORM
REGIONAL ADMINISTRATORS: in the top chart section of the invoice/claims form please pre-fill contact information prior to sending form to Child Care/Early Education Programs (the area Date Form Received should be filled in after the claim is received from the program).
EARLY CHILD CARE PROGRAM: 1. In the top chart area - Fill in your program information. (Authorizer, Title, Position, Address, etc.) 2. There is also a signature required for the authorized person to sign and date the form. Claims will not be processed without a valid signature. 3. List the service period for which these claim applies and enter the date the form was completed. 4. In the next section, complete the information for EACH child in your program that has a Pathway I Early Learning Scholarship that you are requesting reimbursement for. You may attach an additional form (located on the last page of this document) if you need to submit more claims.
- Enter an invoice number in this format: 9/2013 (m/yyyy). However, if recipient received an identifier number, please indicate that in the invoice number area also for example: 9/2013/identifier number. This is useful for tracking purposes. - Enter the participating Family/Parent or Legal Guardian by first, last name and date of birth (m/d/yyyy). - Enter the child(ren) by first, last name and date of birth (m/d/yyyy). One child per line. - Follow the specific instructions to enter information in the bottom row (in the shaded boxes). An example is provided (in green font)
- Under column “A”: Program Tuition - enter the cost for that child to attend during the service period listed. For families receiving CCAP, list the full cost prior to any deductions (do not deduct the family’s copayment or the amount paid by CCAP). For School Readiness programs, use cost per child determined by your school district. Please reference “Early Learning Scholarships in Minnesota; Information for Early Care and Education Providers” (memo date 10/12/12).
- Under column “B”: Additional Program Fees - fill in any additional parent fees for the current service period. Fees may include charges for field trips, uniforms, activities, or other fees that are charged. Note: If a provider charges a fee to families with scholarships, they must charge the same fee to families without scholarships that receive the same service.
- Under column “C”: o If you are Head Start or School Readiness program SKIP this column. o If you are a Child Care Program and if the child is receiving Child Care Assistance, fill in the amount that your program have received or expects to receive for this service period.
- Under column “D”: o If you are Head Start or School Readiness program SKIP this column. o If you are a Child Care Program and if you have received other sources of payment for this child during this service period, fill in that dollar amount received.
Early Learning Scholarship Invoice/Claim Form 2014-2015 - Under column “E”: Fill in the total amount that is requested for Early Learning Scholarships. To determine this amount: o If you are Head Start or School Readiness program add up columns A and B (Program Tuition and Additional Program Fees). o If you are a Child Care Program add up columns A and B (Program Tuition and Additional Program Fees) and subtract columns C and D (CCAP and other sources of payment). For families receiving CCAP, the amount requested may include the family’s copayment, the difference between the provider’s rates and CCAP maximum rates, and other costs not paid by CCAP.
- Under column “F”, enter number of days the child was absent - This information is required for evaluation purposes only. It will not affect the scholarship amount that you receive.
- Under column “G”, enter number of days the child attended - This information is required for evaluation purposes only. It will not affect the scholarship amount that you receive.
Note: - School Readiness, Head Start or Child Care Programs with a current Three or Four-Star Parent Aware rating are eligible for up to $5,000 per eligible child per year. - Child Care Programs with a One or Two-Star rating are eligible for $4,000 per eligible child per year, and - Programs that have signed a Parent Aware Participation Agreement but have not yet received a rating form are eligible for up to $3,000 per eligible child per year. - Your assigned Administrator identified on cover page of invoice/claims form will track the amount available for each child. - If the amount requested exceeds the amount remaining in the child’s Scholarship, reimbursement will only be made up to the maximum of the Scholarship award granted
Early Learning Scholarship Invoice/Claim Form 2014-2015 Participating Participating A B C D E F G FAMILY CHILD(ren) Invoice Print first, last name, Enter first, last name, Program Additional Child care Other Early Number of Number of Number: and date of birth and date of birth (DOB) Tuition Program Assistance Sources Learning days child days child (example) Fees Program of Payment Scholarship was absent attended (CCAP) Received Amount Troy Smith, 6/19/2010 (m/yyyy) DOB: Billed/Paid Requested (m/d/yyyy) (A+B) – (C+D) Child 1: $ $ $ $ $ DOB: Child 2: $ $ $ $ $ DOB: Please indicate (using codes in the shaded boxes to the right ) ⇢ #1 = an increase in access to quality ECE programs. #1 applies to Child # , # if the EL Scholarship resulted in either #1-5 and for which child it #2 = an increase in # of children served. #2 applies to Child # , # applied: #3 = an increase in child’s time in the program. #3 applies to Child # , # Example: #1 applies to child #2 #4 = covers cost of parent fees, charges for attendance. #4 applies to Child # , # #5 = additional services (i.e. transportation, etc.) #5 applies to Child # , #
Participating Participating A B C D E F G FAMILY CHILD(ren) Invoice Print first, last name, Enter first, last name, Program Additional Child care Other Early Number of Number of Number: and date of birth and date of birth (DOB) Tuition Program Assistance Sources Learning days child days child (example) Fees Program of Payment Scholarship was absent attended (CCAP) Received Amount Troy Smith, 6/19/2010 (m/yyyy) DOB: Billed/Paid Requested (m/d/yyyy) (A+B) – (C+D) Child 1: $ $ $ $ $ DOB: Child 2: $ $ $ $ $ DOB: Please indicate (using codes in the shaded boxes to the right ) ⇢ #1 = an increase in access to quality ECE programs. #1 applies to Child # , # if the EL Scholarship resulted in either #1-5 and for which child it #2 = an increase in # of children served. #2 applies to Child # , # applied: #3 = an increase in child’s time in the program. #3 applies to Child # , # Example: #1 applies to child #2 #4 = covers cost of parent fees, charges for attendance. #4 applies to Child # , # #5 = additional services (i.e. transportation, etc.) #5 applies to Child # , #
Early Learning Scholarship Invoice/Claim Form 2014-2015