Laparoscopic Right Hemicolectomy - Yee last updated June 2007
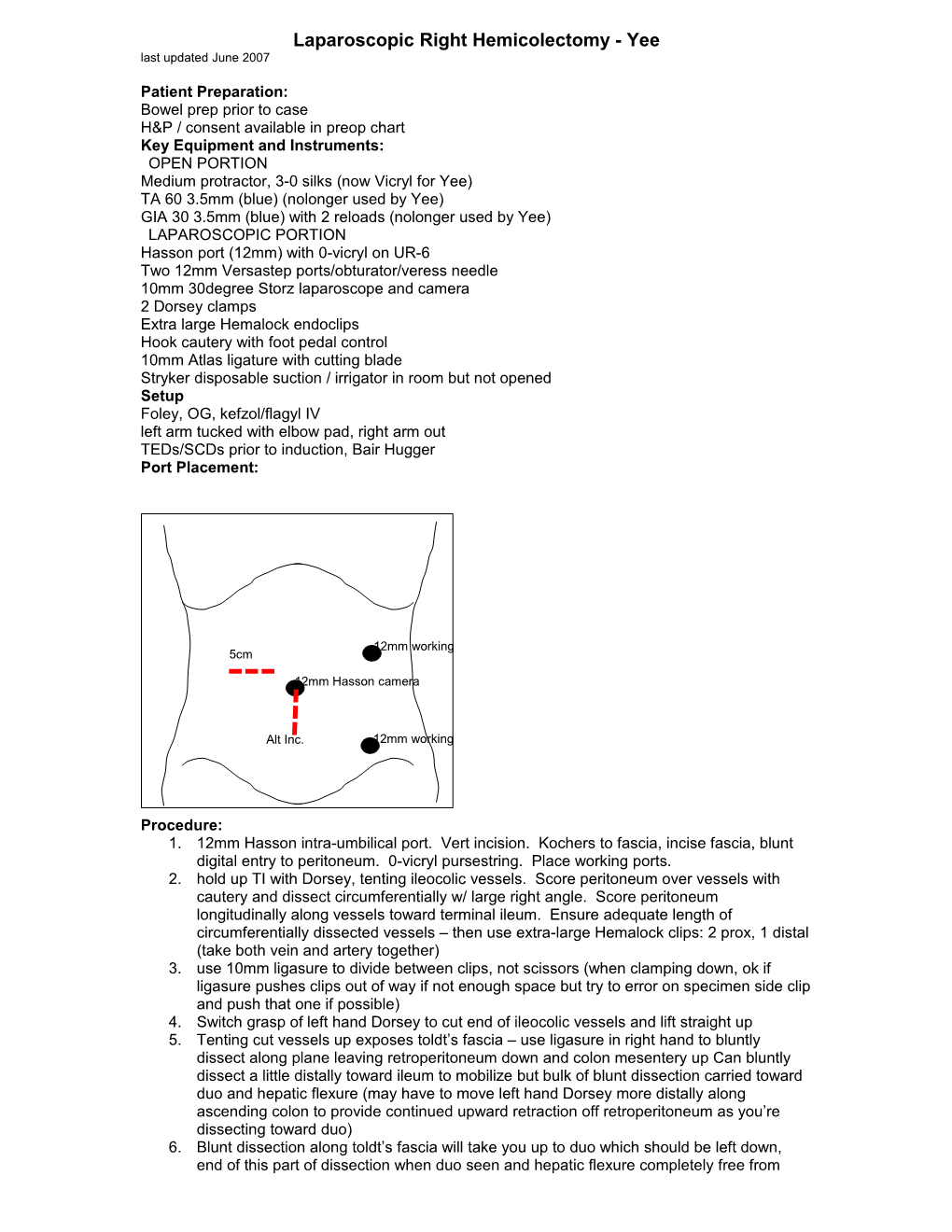
Patient Preparation: Bowel prep prior to case H&P / consent available in preop chart Key Equipment and Instruments: OPEN PORTION Medium protractor, 3-0 silks (now Vicryl for Yee) TA 60 3.5mm (blue) (nolonger used by Yee) GIA 30 3.5mm (blue) with 2 reloads (nolonger used by Yee) LAPAROSCOPIC PORTION Hasson port (12mm) with 0-vicryl on UR-6 Two 12mm Versastep ports/obturator/veress needle 10mm 30degree Storz laparoscope and camera 2 Dorsey clamps Extra large Hemalock endoclips Hook cautery with foot pedal control 10mm Atlas ligature with cutting blade Stryker disposable suction / irrigator in room but not opened Setup Foley, OG, kefzol/flagyl IV left arm tucked with elbow pad, right arm out TEDs/SCDs prior to induction, Bair Hugger Port Placement:
12mm working 5cm
12mm Hasson camera
Alt Inc. 12mm working
Procedure: 1. 12mm Hasson intra-umbilical port. Vert incision. Kochers to fascia, incise fascia, blunt digital entry to peritoneum. 0-vicryl pursestring. Place working ports. 2. hold up TI with Dorsey, tenting ileocolic vessels. Score peritoneum over vessels with cautery and dissect circumferentially w/ large right angle. Score peritoneum longitudinally along vessels toward terminal ileum. Ensure adequate length of circumferentially dissected vessels – then use extra-large Hemalock clips: 2 prox, 1 distal (take both vein and artery together) 3. use 10mm ligasure to divide between clips, not scissors (when clamping down, ok if ligasure pushes clips out of way if not enough space but try to error on specimen side clip and push that one if possible) 4. Switch grasp of left hand Dorsey to cut end of ileocolic vessels and lift straight up 5. Tenting cut vessels up exposes toldt’s fascia – use ligasure in right hand to bluntly dissect along plane leaving retroperitoneum down and colon mesentery up Can bluntly dissect a little distally toward ileum to mobilize but bulk of blunt dissection carried toward duo and hepatic flexure (may have to move left hand Dorsey more distally along ascending colon to provide continued upward retraction off retroperitoneum as you’re dissecting toward duo) 6. Blunt dissection along toldt’s fascia will take you up to duo which should be left down, end of this part of dissection when duo seen and hepatic flexure completely free from underlying duo (At this point you can take middle colic vessels w/ ligasure if seen or you can do this after hepatic flexure mobilized or extracorporally) 7. Left hand Dorsey pull down transverse colon toward toes just beyond hepatic flexure, open lesser sac with ligasure 8. Continue dissection with ligasure toward flexure and take down hepatic flexure with ligasure 9. Continue dissection around corner moving more proximally back toward cecum and use ligasure to take down White line of toldt. May have to switch hands at cecum using Dorsey in right and hook cautery in left to get last bit of cecum mobilized 10. 5cm incision RMQ or just expand umbo incision inferiorly. medium protractor. 11. Deliver right colon. staple TI and Tcolon. specimen off. side-to-side stapled ileocolostomy. Alice x3, TA enterotomies. lembert TA staple line with 3-0 silk. (Laurence now uses non-crushing bowel clamps and divides bowel with knife; hand sewn end to end using 3-0 vicryl pop at each corner, lay in middle lembert, then divide gaps each with one more 3-0 vicryl lembert for total of 5 lemberts along posterior wall, inner layer approximated w/ 4-0 PDS double arm, place in middle and run back wall in either direction, Connell anterior wall; lay in additional lembert 3-0 vicryl pops to hide PDS stitch anteriorly – no set number unlike posterior wall) 12. 0 PDS for peritoneum / posterior rectus sheath. 0 PDS for anterior rectus sheath (For midline incision, use 1 running 0 PDS stich to reapproximate fascia) 13. 4-0 monocryl skin
Postoperative Care: kefzol/flagyl 24h Clears POD1 ADAT POD2