ADD/ADHD Individualized Healthcare Plan (IHCP)
Student: ______Date of Birth: ______Grade: ______Teacher/Staff Contact Person: ______
Student’s Secondary Health Concerns (if applicable): ______
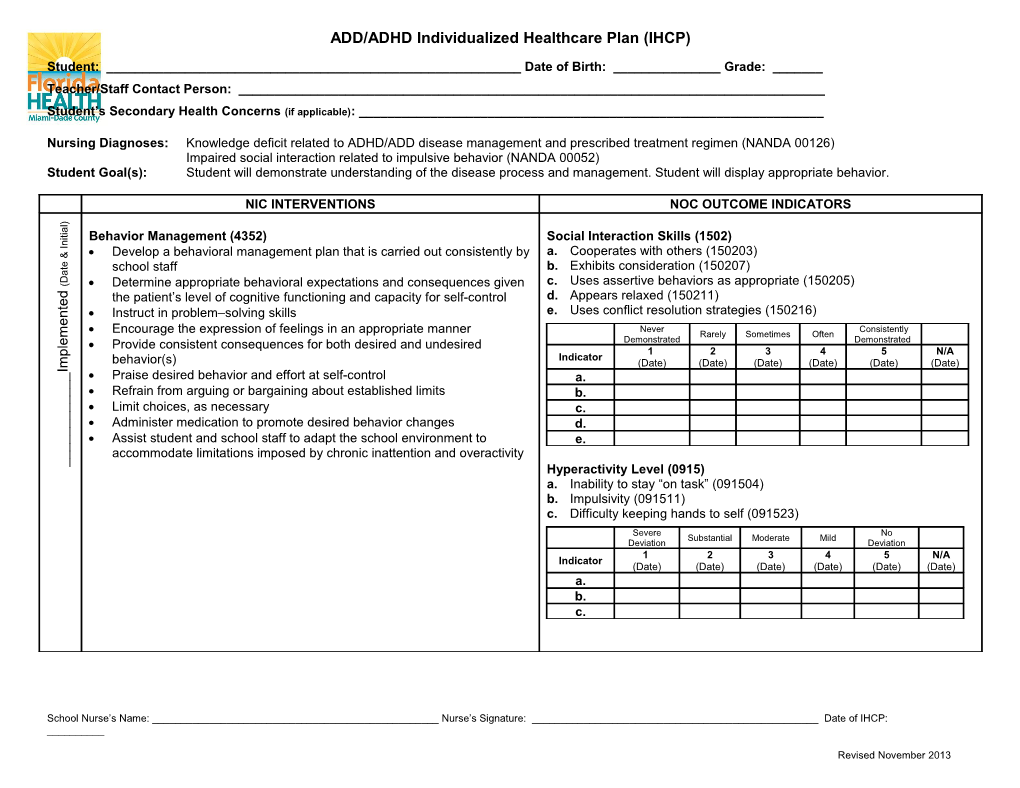
Nursing Diagnoses: Knowledge deficit related to ADHD/ADD disease management and prescribed treatment regimen (NANDA 00126) Impaired social interaction related to impulsive behavior (NANDA 00052) Student Goal(s): Student will demonstrate understanding of the disease process and management. Student will display appropriate behavior.
NIC INTERVENTIONS NOC OUTCOME INDICATORS
) l a i t i Behavior Management (4352) Social Interaction Skills (1502) n I a. Cooperates with others (150203)
& Develop a behavioral management plan that is carried out consistently by
e t school staff b. Exhibits consideration (150207) a D
( Determine appropriate behavioral expectations and consequences given c. Uses assertive behaviors as appropriate (150205)
d the patient’s level of cognitive functioning and capacity for self-control d. Appears relaxed (150211) e t e. Uses conflict resolution strategies (150216) n Instruct in problem–solving skills e Encourage the expression of feelings in an appropriate manner Never Consistently
m Rarely Sometimes Often Demonstrated Demonstrated e
l Provide consistent consequences for both desired and undesired
p 1 2 3 4 5 N/A behavior(s) Indicator
m (Date) (Date) (Date) (Date) (Date) (Date) I
_ Praise desired behavior and effort at self-control a. _
_ Refrain from arguing or bargaining about established limits b. _
_ Limit choices, as necessary c. _
_ Administer medication to promote desired behavior changes d. _
_ Assist student and school staff to adapt the school environment to e. _
_ accommodate limitations imposed by chronic inattention and overactivity _ Hyperactivity Level (0915) a. Inability to stay “on task” (091504) b. Impulsivity (091511) c. Difficulty keeping hands to self (091523) Severe No Substantial Moderate Mild Deviation Deviation 1 2 3 4 5 N/A Indicator (Date) (Date) (Date) (Date) (Date) (Date) a. b. c.
School Nurse’s Name: ______Nurse’s Signature: ______Date of IHCP: ______
Revised November 2013 ) l a i t i n I
&
e t a D (
d e t n e m e l
p ADD/ADHD Individualized Healthcare Plan (IHCP) Student Name: ______m I _
_ Health Education (5510) Knowledge: Disease Process (1803) _ a. Specific disease process (180302) _ Determine current health knowledge and lifestyle behavior of student and _ b. Signs and symptoms (180306) _ family _ c. Potential complications of disease (180309) _ Emphasize importance of healthy patterns of eating, sleeping, exercising, _ d. Precautions to prevent complications (180311)
_ etc. _ No Extensive _ Limited Moderate Substantial Knowledge Knowledge Teaching: Disease Process (5602) 1 2 3 4 5 N/A Indicator Review & acknowledge student’s knowledge about condition (Date) (Date) (Date) (Date) (Date) (Date) Describe the disease process, and common signs and symptoms of the a. disease, as appropriate b. Discuss lifestyle changes that may be required to prevent future c. complications, and/or control the disease process d. _ _
_ Delegation (7650) Caregiver Performance: Direct Care (2205) _
_ Determine the student’s care that needs to be completed a. Knowledge of treatment regimen (220504) _
_ Identify the potential for harm b. Performance of procedure (220516) _
_ Evaluate the competency and training of unlicensed assistive personnel c. Surveillance of health status of student (220508) _
_ (UAP) d. Confidence performing needed task (220513) _
Not Totally
) Determine the level of supervision needed for the specific delegated
l Slightly Moderately Substantially
a Adequate Adequate i
t intervention or activity i
n 1 2 3 4 5 N/A I
Indicator Follow-up with UAP on regular basis to evaluate their progress for (Date) (Date) (Date) (Date) (Date) (Date) &
e t completing the specific task a. a
D Evaluate the outcome of the delegated intervention or activity ( b.
d Develop emergency care plan, as appropriate c. e t
n d. e m e l p m I
School Nurse’s Name: ______Nurse’s Signature: ______Date of IHCP: ______
Revised November 2013 ADD/ADHD Individualized Healthcare Plan (IHCP) Student Name: ______) l a i t i n
I Medication Management (2380) Knowledge: Medication (1808)
& Determine student’s ability to self-medicate, as appropriate a. Identification of the correct name of medication (180802) e t
a Monitor effectiveness of the medication administration modality b. Medication side effect (180805) D ( Monitor student for therapeutic effect of the medication c. Correct use of prescribed medication (180810) d
e d. Proper medication storage (180812) t Determine the student’s and UAP’s knowledge about medication
n e. Proper disposal of medication (180815)
e Teach UAP the method of drug administration, as appropriate
m No Extensive Instruct student when to seek medical attention Limited Moderate Substantial e
l Knowledge Knowledge p Review with the student and UAP strategies for managing medication 1 2 3 4 5 N/A
m Indicator
I regimen (Date) (Date) (Date) (Date) (Date) (Date) _
_ a. _
_ b. _
_ c. _
_ d. _
_ e. _ _ _ _
_ Medication Administration (2300) Medication Response (2301) _
_ Verify medication order before administration a. Expected therapeutic effects (230101) _ _
Monitor student for therapeutic effect of the medication Severely Not )
l Substantially Moderately Mildly
a Compromised Compromised i
t Monitor student for adverse effects, toxicity, and interactions of the i
n 1 2 3 4 5 N/A I administered medication Indicator &
(Date) (Date) (Date) (Date) (Date) (Date) e t
a a. D (
d e t n e m e l p m I
School Nurse’s Name: ______Nurse’s Signature: ______Date of IHCP: ______
Revised November 2013 ADD/ADHD Individualized Healthcare Plan (IHCP) Student Name: ______) l a i t i n
I Student Health Status (2005)
& a. Physical health (200501) e t
a b. Mental health (200502) D ( c. School attendance (200503) d
e d. Readiness to learn (200504) t
n e. Return to class after visit to health office (200508) e
m f. Reports to the health office for medications at appropriate time e l (200511) p
m g. Participation in self-care activities (200514) I
_ h. Students with chronic illness or special needs managed according to _
_ IHCP/IEP (200515) _
_ i. Participation in physical activities (200519) _
_ j. Healthy dietary habits (200523) _
_ Severely Not Substantially Moderately Mildly _ Compromised Compromised _ 1 2 3 4 5 N/A Indicator (Date) (Date) (Date) (Date) (Date) (Date) a. b. c. d. e. f. g. h. i. j.
School Nurse’s Name: ______Nurse’s Signature: ______Date of IHCP: ______
Revised November 2013