Head Shaking Nystagmus
Timothy C. Hain, MD
References:
1. Hain TC, Fetter M, Zee DS: Head-shaking nystagmus in unilateral peripheral vestibular lesions. American J. Otolaryngology., 8:36-47, 1987. 2. Wei D, Hain TC, Proctor L: Head-shaking nystagmus: associations with canal paresis and hearing loss. Acta Otology. 108: 362-367, 1989. 3. Hain TC, Spindler J: Head-Shaking Nystagmus. in The Vestibulo- Ocular Reflex and Vertigo (Ed. Sharpe JA, Barber HO), Raven, 1993
Head-shaking nystagmus is the nystagmus that follows sinusoidal movement of the head. There are three variants: Horizontal head-shaking -- rotation of the head in the horizontal plane, vertical head- shaking -- rotation in the vertical plane, and circular head-shaking -- rotation of the head so that the nose traces out a circle in the coronal plane. The usual duration is 20 cycles, aiming for a horizontal or vertical movement of about 30-45 degrees, and a frequency of roughly one cycle/sec.
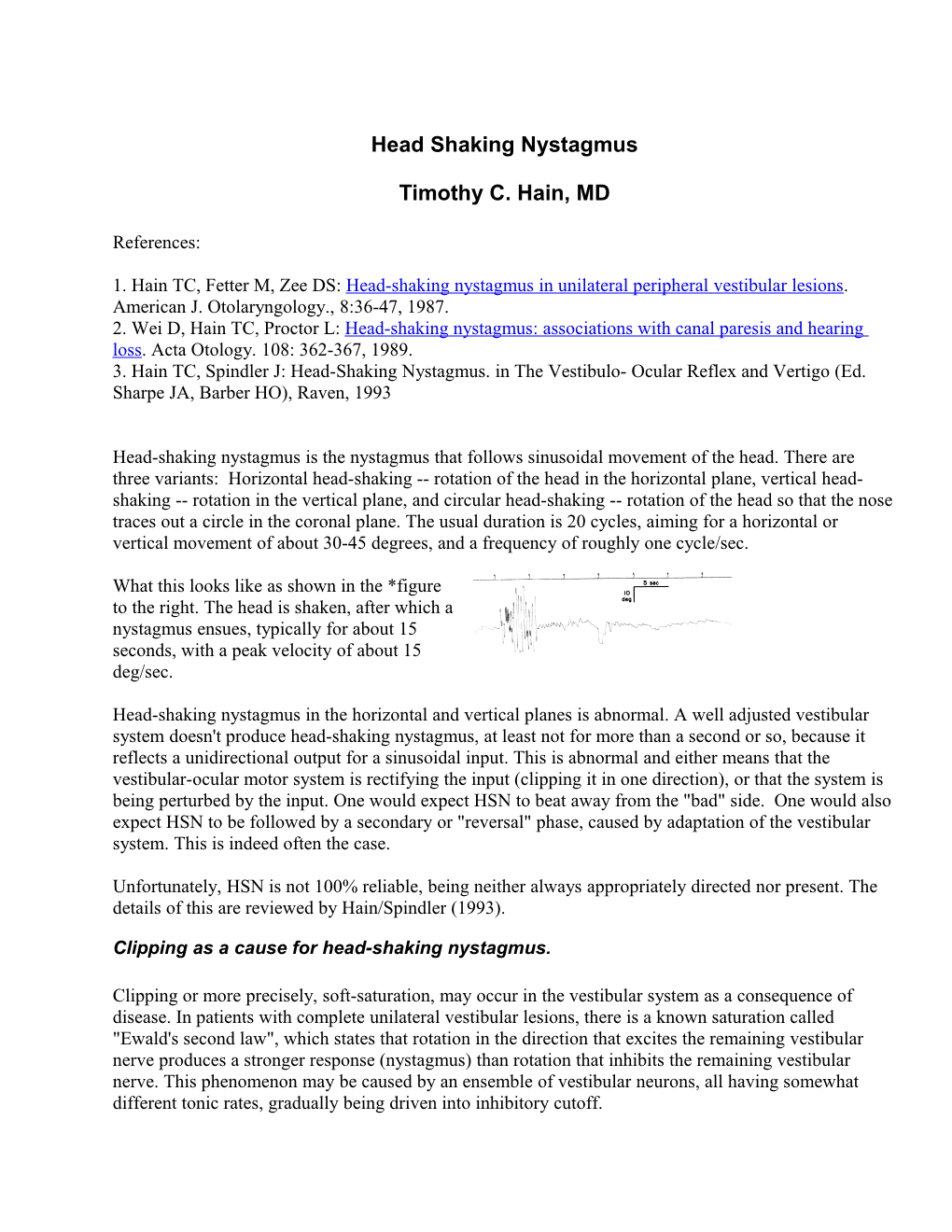
What this looks like as shown in the *figure to the right. The head is shaken, after which a nystagmus ensues, typically for about 15 seconds, with a peak velocity of about 15 deg/sec.
Head-shaking nystagmus in the horizontal and vertical planes is abnormal. A well adjusted vestibular system doesn't produce head-shaking nystagmus, at least not for more than a second or so, because it reflects a unidirectional output for a sinusoidal input. This is abnormal and either means that the vestibular-ocular motor system is rectifying the input (clipping it in one direction), or that the system is being perturbed by the input. One would expect HSN to beat away from the "bad" side. One would also expect HSN to be followed by a secondary or "reversal" phase, caused by adaptation of the vestibular system. This is indeed often the case.
Unfortunately, HSN is not 100% reliable, being neither always appropriately directed nor present. The details of this are reviewed by Hain/Spindler (1993).
Clipping as a cause for head-shaking nystagmus.
Clipping or more precisely, soft-saturation, may occur in the vestibular system as a consequence of disease. In patients with complete unilateral vestibular lesions, there is a known saturation called "Ewald's second law", which states that rotation in the direction that excites the remaining vestibular nerve produces a stronger response (nystagmus) than rotation that inhibits the remaining vestibular nerve. This phenomenon may be caused by an ensemble of vestibular neurons, all having somewhat different tonic rates, gradually being driven into inhibitory cutoff. Patients with unilateral vestibular loss do indeed exhibit head-shaking nystagmus. In the adjacent figure adapted from Hain et al, 1997, a strong HSN is illustrated in patient with unilateral vestibular loss caused by an acoustic neuroma. As mentioned above, HSN generally beats away from the "bad" side and has a reversal phase. One would also expect HSN to be followed by a secondary or "reversal" phase, caused by adaptation of the vestibular system.
HSN is somewhat erratic. As illustrated by the figure below on the left, in patients with complete unilateral loss, while the direction is consistent, the size and duration varies.
In general, HSN should result from any vestibular nonlinearity , whether it be peripheral or central, and could also result from interactions from neck afferents which are, of course, also stimulated by head-shaking.
In theory, for HSN to be generated, the nonlinearity must also be accompanied by some dynamics to average and retain the clipped input. In the past we have proposed that the velocity storage mechanism performs this function.
Perturbation as a cause of HSN. Another possible source of head-shaking nystagmus is simply a response of the system to any perturbation. In the old German literature, this was called "latent nystagmus". From a systems analysis perspective, this also derives from nonlinearity, but it need not necessarily scale with the size of the input
Situations where it seems likely that HSN is simply a result of perturbation are generally central ones. In the figure on the left, an extremely powerful HSN is produced, which is inconsistent with the amount of nystagmus produced in complete peripheral vestibular lesions. This could in theory be either due to a more drastic central nonlinearity in this patient with a vestibular nucleus infarct, or from perturbation. In the figure above to the right an example of a strong head-shaking nystagmus is given where the reversal phase is larger than the primary phase. This may be an example of HSN caused by a perturbation. A model of this nystagmus was proposed in Hain and Spindler, 1993 and is shown in the figure above. A simulation was also displayed..
Circular head-shaking nystagmus.
An interesting "parlor trick" is to move the head in a circular fashion, so that the nose traces out a circle in the frontal plane. It this is done for 10 cycles fairly briskly, on stopping a very brisk rotatory nystagmus can be seen with frenzel goggles or any other method of observing the eyes.
Unlike the horizontal and vertical HSN discussed above, this so-called "circular HSN", first described by Hain and Spindler (1993), occurs quite reproducably in normal individuals. It can be shown (with some effort) that circular-HSN is a consequence of geometry. In this type of movement, the head is in- effect rotating about the front-back axis of the head (without getting twisted off !). When the head-stops, what ensues is simply a post-rotatory nystagmus.
There seems to be relatively little use for this observation so far, but perhaps it may be productively applied to testing of the torsional VOR in the future, once eye-movement transducers become available that can non-invasively register rotatory eye movements.