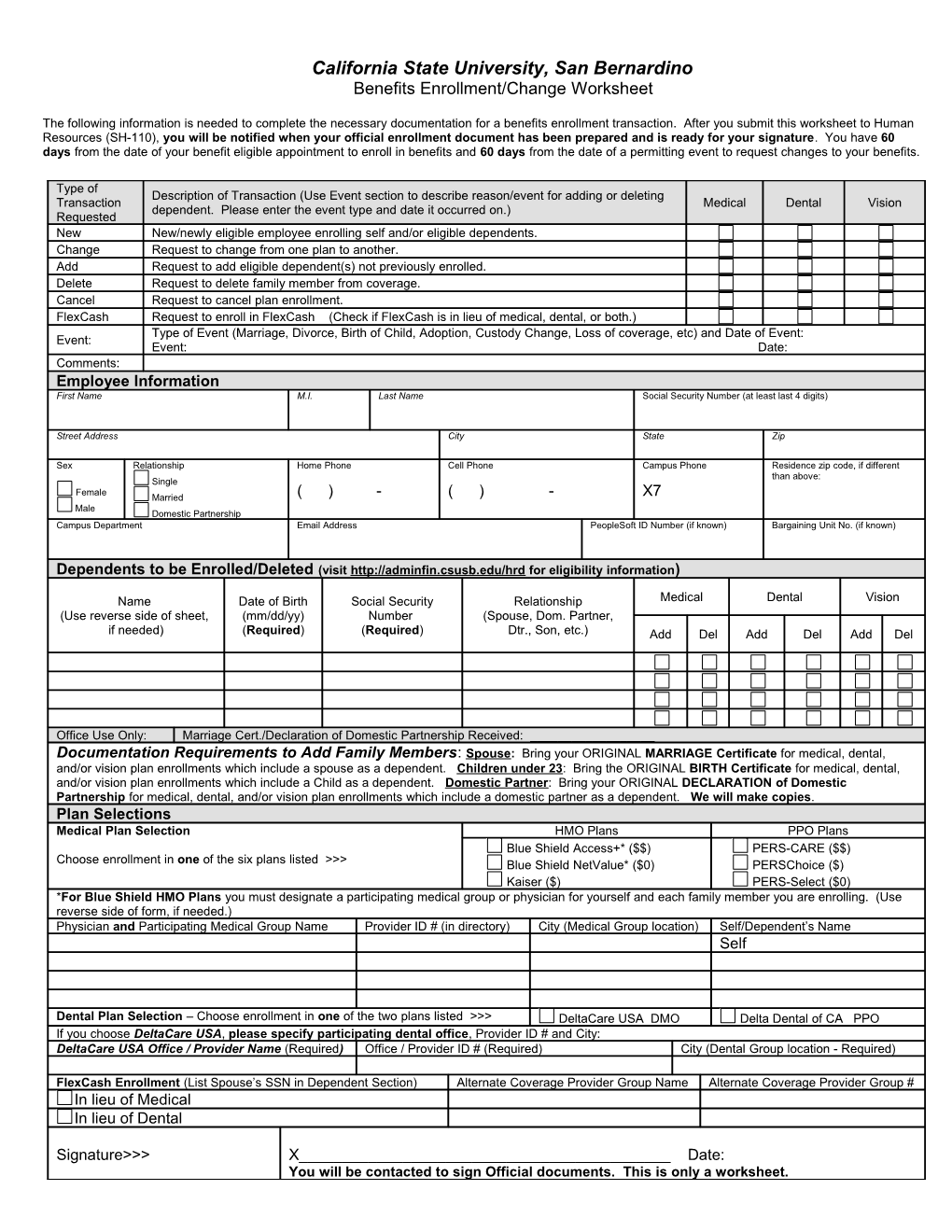
California State University, San Bernardino Benefits Enrollment/Change Worksheet
The following information is needed to complete the necessary documentation for a benefits enrollment transaction. After you submit this worksheet to Human Resources (SH-110), you will be notified when your official enrollment document has been prepared and is ready for your signature. You have 60 days from the date of your benefit eligible appointment to enroll in benefits and 60 days from the date of a permitting event to request changes to your benefits.
Type of Description of Transaction (Use Event section to describe reason/event for adding or deleting Transaction Medical Dental Vision dependent. Please enter the event type and date it occurred on.) Requested New New/newly eligible employee enrolling self and/or eligible dependents. Change Request to change from one plan to another. Add Request to add eligible dependent(s) not previously enrolled. Delete Request to delete family member from coverage. Cancel Request to cancel plan enrollment. FlexCash Request to enroll in FlexCash (Check if FlexCash is in lieu of medical, dental, or both.) Type of Event (Marriage, Divorce, Birth of Child, Adoption, Custody Change, Loss of coverage, etc) and Date of Event: Event: Event: Date: Comments: Employee Information First Name M.I. Last Name Social Security Number (at least last 4 digits)
Street Address City State Zip
Sex Relationship Home Phone Cell Phone Campus Phone Residence zip code, if different than above: Single Female Married ( ) - ( ) - X7 Male Domestic Partnership Campus Department Email Address PeopleSoft ID Number (if known) Bargaining Unit No. (if known)
Dependents to be Enrolled/Deleted (visit http://adminfin.csusb.edu/hrd for eligibility information)
Name Date of Birth Social Security Relationship Medical Dental Vision (Use reverse side of sheet, (mm/dd/yy) Number (Spouse, Dom. Partner, if needed) (Required) (Required) Dtr., Son, etc.) Add Del Add Del Add Del
Office Use Only: Marriage Cert./Declaration of Domestic Partnership Received: ______Documentation Requirements to Add Family Members: Spouse: Bring your ORIGINAL MARRIAGE Certificate for medical, dental, and/or vision plan enrollments which include a spouse as a dependent. Children under 23: Bring the ORIGINAL BIRTH Certificate for medical, dental, and/or vision plan enrollments which include a Child as a dependent. Domestic Partner: Bring your ORIGINAL DECLARATION of Domestic Partnership for medical, dental, and/or vision plan enrollments which include a domestic partner as a dependent. We will make copies. Plan Selections Medical Plan Selection HMO Plans PPO Plans Blue Shield Access+* ($$) PERS-CARE ($$) Choose enrollment in one of the six plans listed >>> Blue Shield NetValue* ($0) PERSChoice ($) Kaiser ($) PERS-Select ($0) *For Blue Shield HMO Plans you must designate a participating medical group or physician for yourself and each family member you are enrolling. (Use reverse side of form, if needed.) Physician and Participating Medical Group Name Provider ID # (in directory) City (Medical Group location) Self/Dependent’s Name Self
Dental Plan Selection – Choose enrollment in one of the two plans listed >>> DeltaCare USA DMO Delta Dental of CA PPO If you choose DeltaCare USA, please specify participating dental office, Provider ID # and City: DeltaCare USA Office / Provider Name (Required) Office / Provider ID # (Required) City (Dental Group location - Required)
FlexCash Enrollment (List Spouse’s SSN in Dependent Section) Alternate Coverage Provider Group Name Alternate Coverage Provider Group # In lieu of Medical In lieu of Dental
Signature>>> X______Date: You will be contacted to sign Official documents. This is only a worksheet. Rev. 01/05/09