DEPARTMENT OF PATHOLOGY SOP name: Basic Semen Analysis Combined Laboratories Plymouth Hospitals N.H.S. Trust SOP No: AND/002
Appendix 3 – Immunology department – Basic Sperm Analysis Record
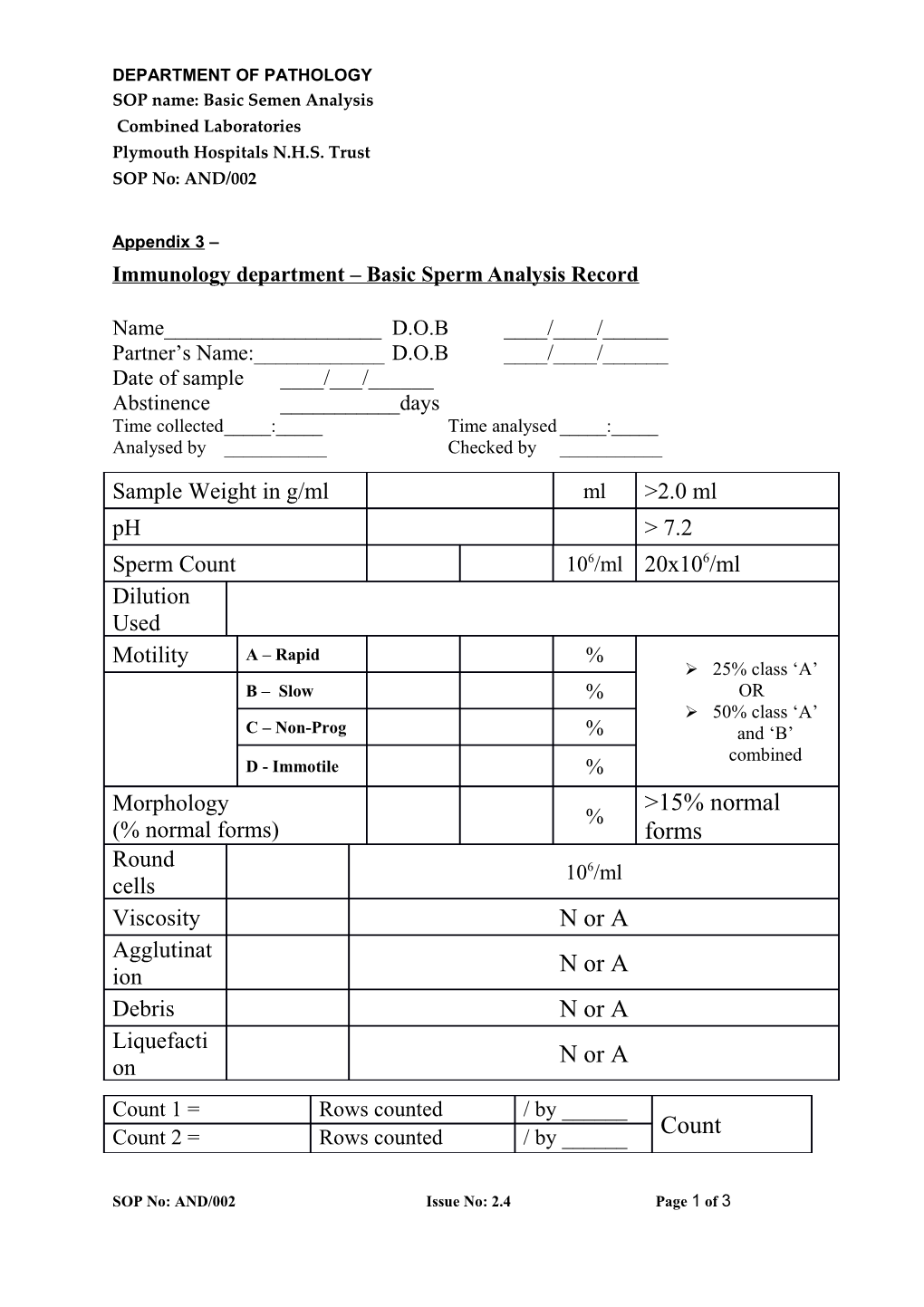
Name______D.O.B ____/____/______Partner’s Name:______D.O.B ____/____/______Date of sample ____/___/______Abstinence ______days Time collected_____:_____ Time analysed _____:_____ Analysed by ______Checked by ______
Sample Weight in g/ml ml >2.0 ml pH > 7.2 Sperm Count 106/ml 20x106/ml Dilution Used Motility A – Rapid % 25% class ‘A’ B – Slow % OR 50% class ‘A’ C – Non-Prog % and ‘B’ combined D - Immotile % Morphology >15% normal % (% normal forms) forms Round 106/ml cells Viscosity N or A Agglutinat N or A ion Debris N or A Liquefacti N or A on Count 1 = Rows counted / by ______Count 2 = Rows counted / by ______Count
SOP No: AND/002 Issue No: 2.4 Page 1 of 3 DEPARTMENT OF PATHOLOGY SOP name: Basic Semen Analysis Combined Laboratories Plymouth Hospitals N.H.S. Trust SOP No: AND/002
Comments:
______Morphology read by:______Morphology checked by: ______Dilution factors are: 1:2 = divide by 10 1:5 = divide by 4 (for 10 squares counted) 1:20 = divide by 1 Seminal Fluid Analysis – Appendix 5 These Tests are undertaken in the immunology section of Derriford Combined Laboratory, Level 06, Derriford Hospital. Please follow the instruction given below: Instructions: Please telephone the Immunology department for an appointment 01752-792293. All appointments run at 9am. No appointment = no testing will be done. Abstain from intercourse or masturbation for 3 to 5 days before producing sample, Smoking should be stopped for 3 months prior to test and kept alcohol intake to a minimum. Clean the penile area before producing the sample by masturbation. Only use the container provided. Do not use a condom. Once the sample is produced keep it at body temperature (inside pocket etc.) and bring it to the laboratory WITHIN AN HOUR OF PRODUCTION. Complete all the details on the form. Deliver to the Immunology Dept, combined laboratory, Level 06, Derriford Hospital, Plymouth. If you are unable to attend your appointment for any reason please ring to cancel your appointment. Please fill this in prior to your appointment: Male partner’s full name: Date of Birth: / / Female partner’s full name: Date of Birth: / / GP and Practice (or referring Doctor: Sample Information: Date of Production: / / Time of production: Abstinence (days): Was there any spillage: Yes/No
SOP No: AND/002 Issue No: 2.4 Page 2 of 3 DEPARTMENT OF PATHOLOGY SOP name: Basic Semen Analysis Combined Laboratories Plymouth Hospitals N.H.S. Trust SOP No: AND/002
If Yes, was the spillage the first part of the sample: Yes/No Please indicate any of the following during the last 3 months:
Illness:
Medications taken:
Alcohol consumption in units in last 48 hours:
Your Signature: Date: / /
SOP No: AND/002 Issue No: 2.4 Page 3 of 3