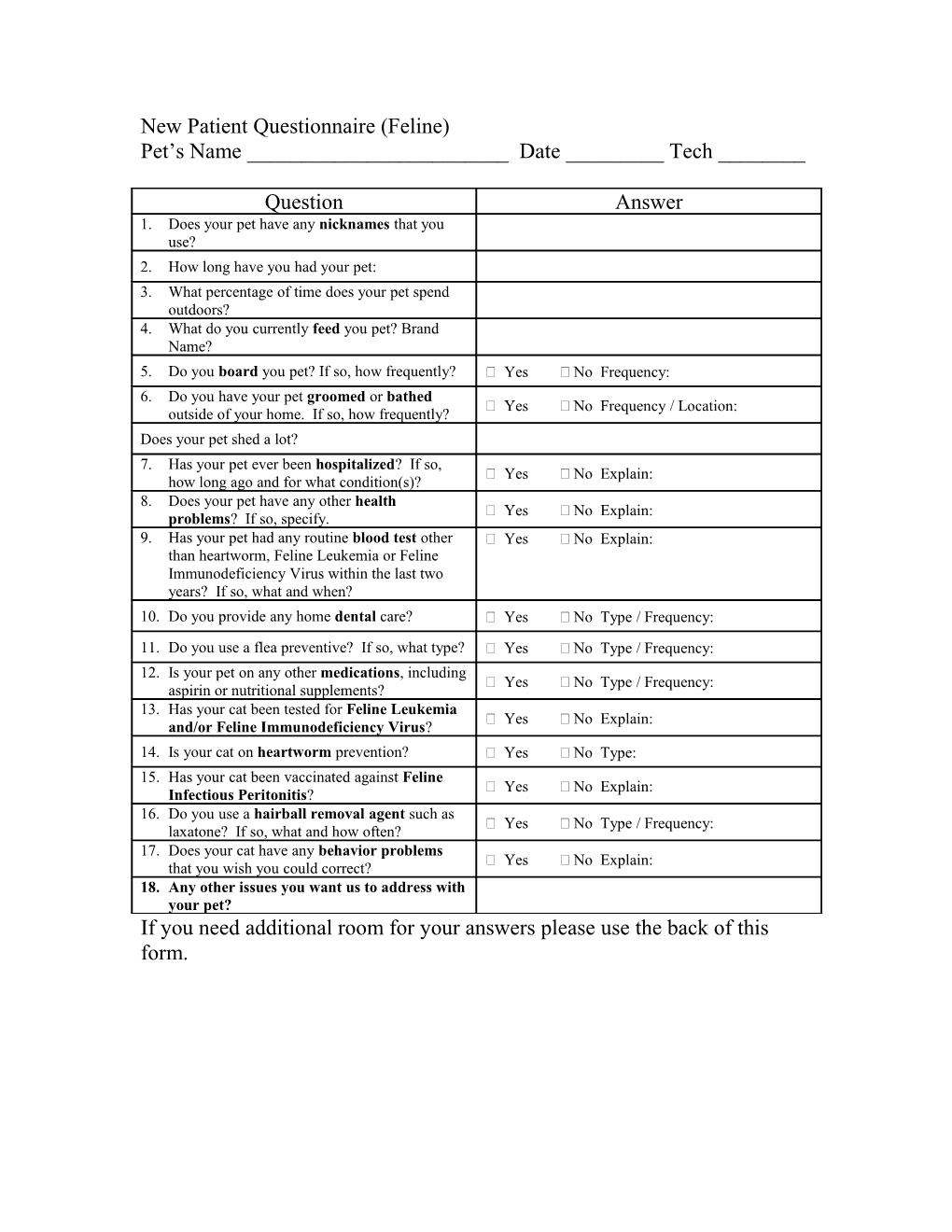
New Patient Questionnaire (Feline) Pet’s Name ______Date ______Tech ______
Question Answer 1. Does your pet have any nicknames that you use? 2. How long have you had your pet: 3. What percentage of time does your pet spend outdoors? 4. What do you currently feed you pet? Brand Name? 5. Do you board you pet? If so, how frequently? Yes No Frequency: 6. Do you have your pet groomed or bathed Yes No Frequency / Location: outside of your home. If so, how frequently? Does your pet shed a lot? 7. Has your pet ever been hospitalized? If so, Yes No Explain: how long ago and for what condition(s)? 8. Does your pet have any other health Yes No Explain: problems? If so, specify. 9. Has your pet had any routine blood test other Yes No Explain: than heartworm, Feline Leukemia or Feline Immunodeficiency Virus within the last two years? If so, what and when? 10. Do you provide any home dental care? Yes No Type / Frequency: 11. Do you use a flea preventive? If so, what type? Yes No Type / Frequency: 12. Is your pet on any other medications, including Yes No Type / Frequency: aspirin or nutritional supplements? 13. Has your cat been tested for Feline Leukemia Yes No Explain: and/or Feline Immunodeficiency Virus? 14. Is your cat on heartworm prevention? Yes No Type: 15. Has your cat been vaccinated against Feline Yes No Explain: Infectious Peritonitis? 16. Do you use a hairball removal agent such as Yes No Type / Frequency: laxatone? If so, what and how often? 17. Does your cat have any behavior problems Yes No Explain: that you wish you could correct? 18. Any other issues you want us to address with your pet? If you need additional room for your answers please use the back of this form.