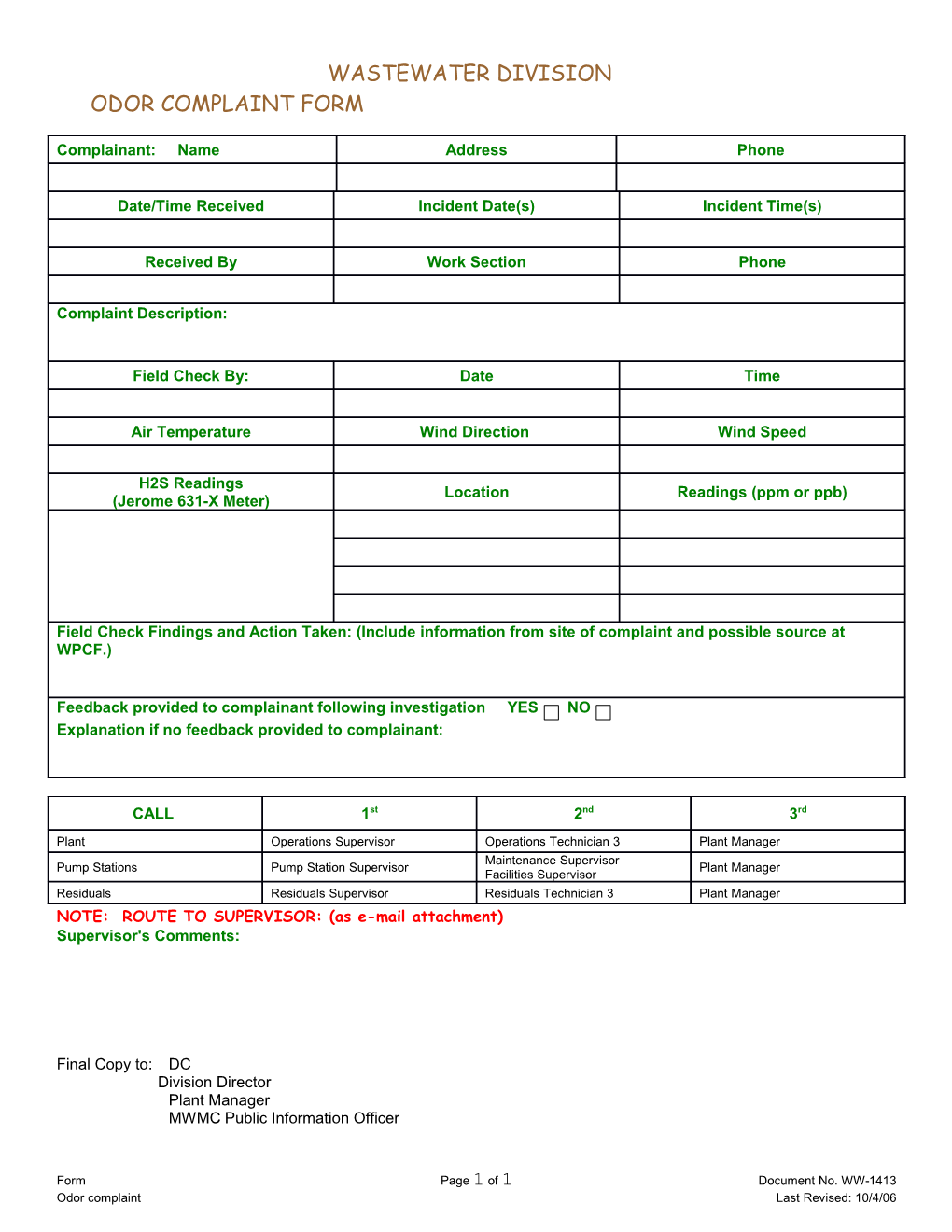
WASTEWATER DIVISION ODOR COMPLAINT FORM
Complainant: Name Address Phone
Date/Time Received Incident Date(s) Incident Time(s)
Received By Work Section Phone
Complaint Description:
Field Check By: Date Time
Air Temperature Wind Direction Wind Speed
H2S Readings Location Readings (ppm or ppb) (Jerome 631-X Meter)
Field Check Findings and Action Taken: (Include information from site of complaint and possible source at WPCF.)
Feedback provided to complainant following investigation YES NO Explanation if no feedback provided to complainant:
CALL 1st 2nd 3rd
Plant Operations Supervisor Operations Technician 3 Plant Manager Maintenance Supervisor Pump Stations Pump Station Supervisor Plant Manager Facilities Supervisor Residuals Residuals Supervisor Residuals Technician 3 Plant Manager NOTE: ROUTE TO SUPERVISOR: (as e-mail attachment) Supervisor's Comments:
Final Copy to: DC Division Director Plant Manager MWMC Public Information Officer
Form Page 1 of 1 Document No. WW-1413 Odor complaint Last Revised: 10/4/06