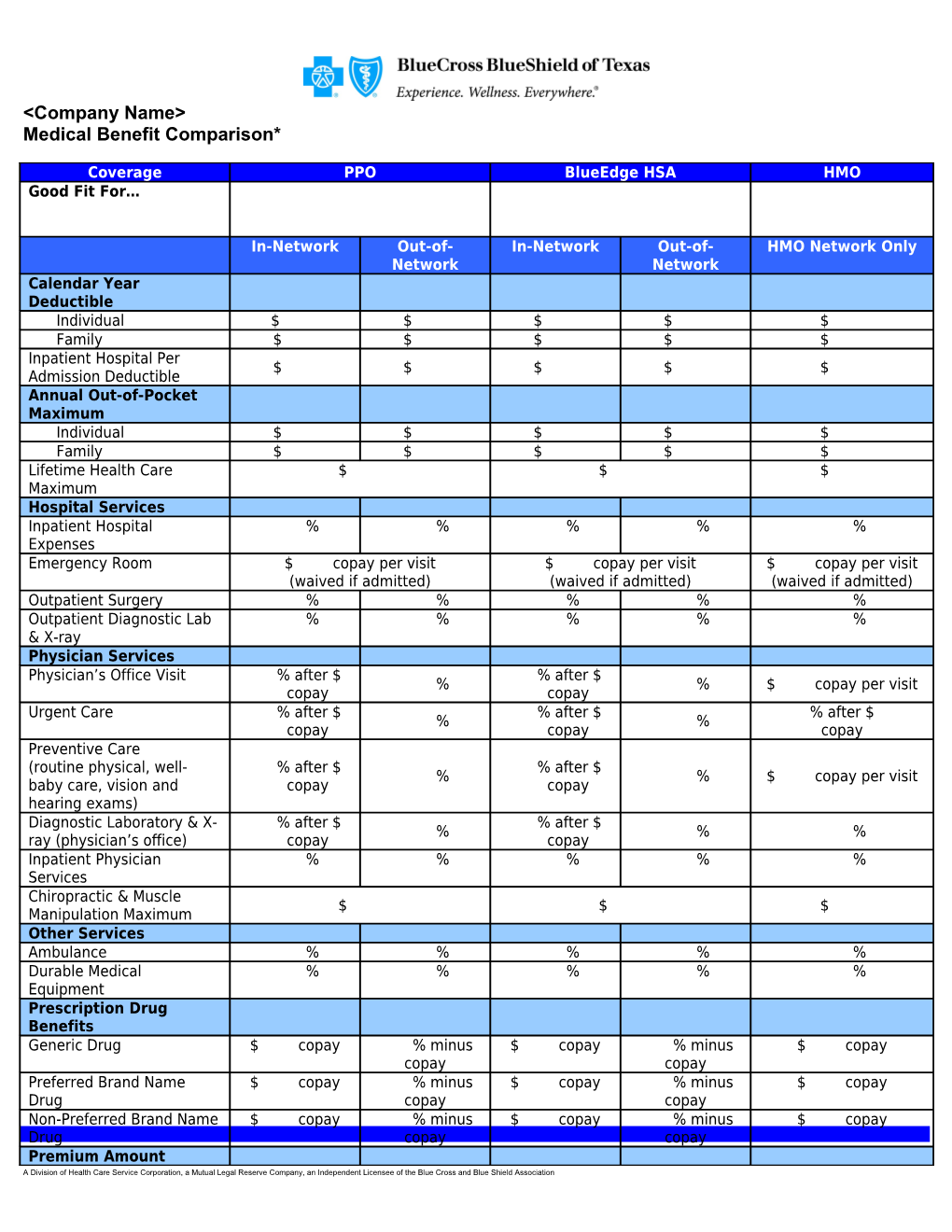
Coverage PPO BlueEdge HSA HMO Good Fit For…
In-Network Out-of- In-Network Out-of- HMO Network Only Network Network Calendar Year Deductible Individual $ $ $ $ $ Family $ $ $ $ $ Inpatient Hospital Per $ $ $ $ $ Admission Deductible Annual Out-of-Pocket Maximum Individual $ $ $ $ $ Family $ $ $ $ $ Lifetime Health Care $ $ $ Maximum Hospital Services Inpatient Hospital % % % % % Expenses Emergency Room $ copay per visit $ copay per visit $ copay per visit (waived if admitted) (waived if admitted) (waived if admitted) Outpatient Surgery % % % % % Outpatient Diagnostic Lab % % % % % & X-ray Physician Services Physician’s Office Visit % after $ % after $ % % $ copay per visit copay copay Urgent Care % after $ % after $ % after $ % % copay copay copay Preventive Care (routine physical, well- % after $ % after $ % % $ copay per visit baby care, vision and copay copay hearing exams) Diagnostic Laboratory & X- % after $ % after $ % % % ray (physician’s office) copay copay Inpatient Physician % % % % % Services Chiropractic & Muscle $ $ $ Manipulation Maximum Other Services Ambulance % % % % % Durable Medical % % % % % Equipment Prescription Drug Benefits Generic Drug $ copay % minus $ copay % minus $ copay copay copay Preferred Brand Name $ copay % minus $ copay % minus $ copay Drug copay copay Non-Preferred Brand Name $ copay % minus $ copay % minus $ copay Drug copay copay Premium Amount A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association Employee Only $ $ $ Employee & Spouse $ $ $ Employee & Child(ren) $ $ $ Family $ $ $ * Percentages apply to allowable amount for eligible expenses after calendar-year deductibles are met.
A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association