Dietary Supplement Labeling Exemption Sample Staff Training Quiz
Directions:
Circle the strength of the Dietary Supplement on the manufacturer’s label.
Based upon the Health Care Provider (HCP) order, document the amount that you would administer.
Transcribe the Health Care Provider order onto the Medication Administration Record.
************************************************************************************************************
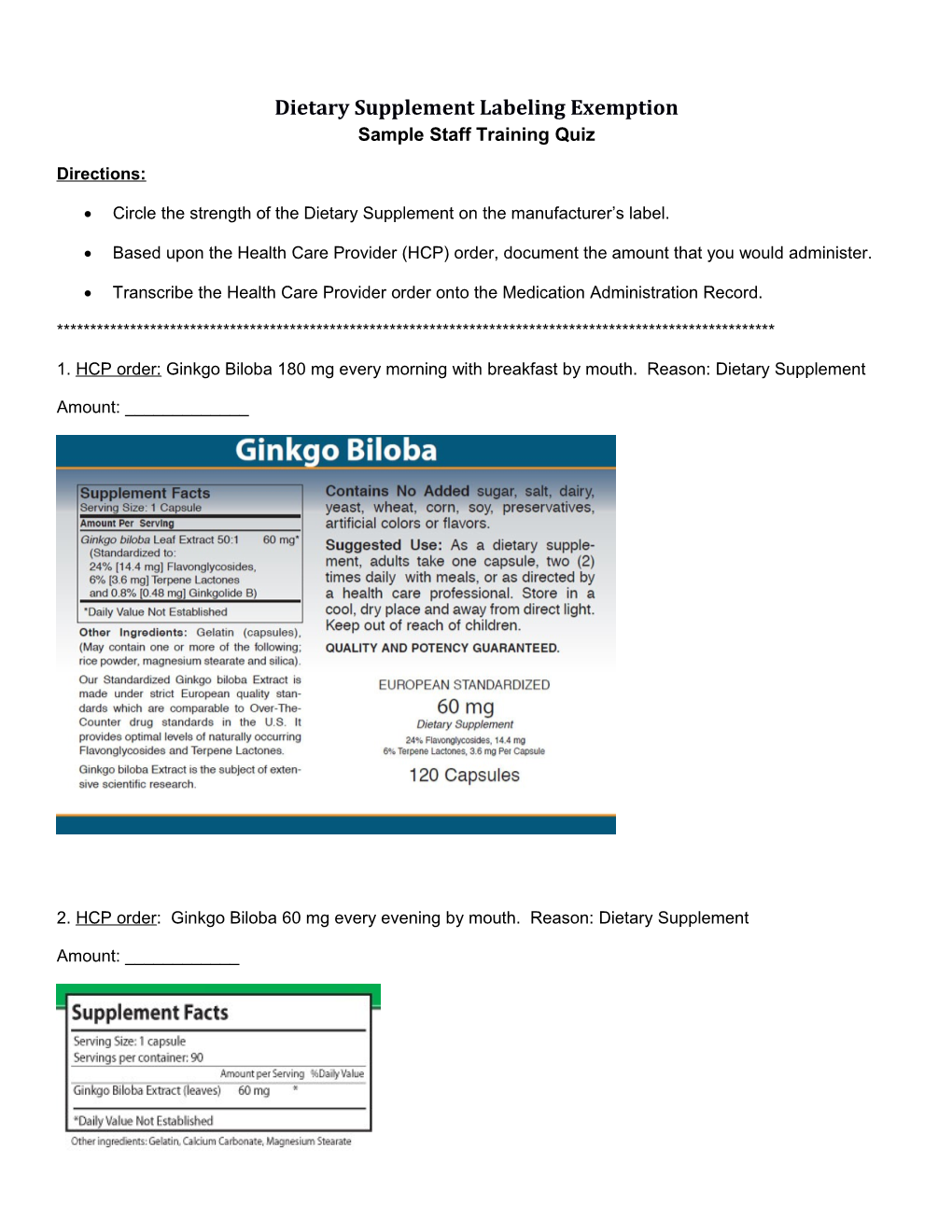
1. HCP order: Ginkgo Biloba 180 mg every morning with breakfast by mouth. Reason: Dietary Supplement
Amount: ______
2. HCP order: Ginkgo Biloba 60 mg every evening by mouth. Reason: Dietary Supplement
Amount: ______3. HCP Order: St. John’s Wort 1400 mg twice a day (with breakfast and supper) by mouth. Reason: Dietary Supplement
Amount: ______
4. HCP Order: Vitamin C 1500 mg twice a day by mouth. Reason: Dietary Supplement
Amount: ______5. HCP Order: Vitamin E 2000 IU daily at bedtime by mouth. Reason: Dietary Supplement
Amount: ______
6. HCP Order: Ascorbic Acid 2000 mg every morning by mouth. Reason: Dietary Supplement
Amount: ______Start Hour 1 3 4 6 7 9 10 12 13 15 16 18 19 21 22 24 25 27 28 2 30 31 9
Stop
Special Instructions:
Reason for Med:
Start Hour 1 3 4 6 7 9 10 12 13 15 16 18 19 21 22 24 25 27 28 2 30 31 9
Stop
Special Instructions:
Reason for Med:
Init Signature Signature Name:
HCP: Program:
Accuracy Check 1 ______Date______Time______Accuracy Check 2 ______Date______Time______Version 7.0 Page __ of __ Pages