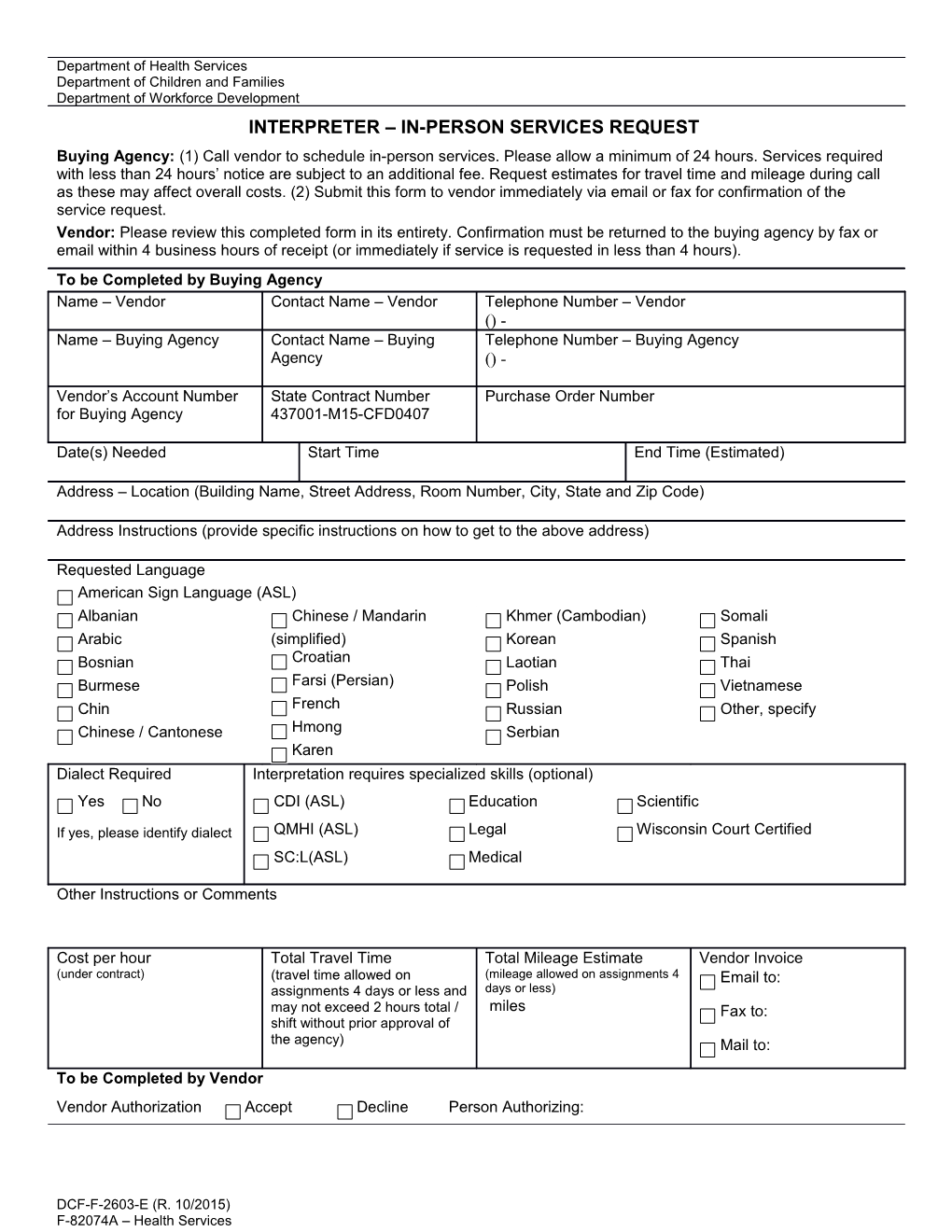
Department of Health Services Department of Children and Families Department of Workforce Development INTERPRETER – IN-PERSON SERVICES REQUEST Buying Agency: (1) Call vendor to schedule in-person services. Please allow a minimum of 24 hours. Services required with less than 24 hours’ notice are subject to an additional fee. Request estimates for travel time and mileage during call as these may affect overall costs. (2) Submit this form to vendor immediately via email or fax for confirmation of the service request. Vendor: Please review this completed form in its entirety. Confirmation must be returned to the buying agency by fax or email within 4 business hours of receipt (or immediately if service is requested in less than 4 hours). To be Completed by Buying Agency Name – Vendor Contact Name – Vendor Telephone Number – Vendor () - Name – Buying Agency Contact Name – Buying Telephone Number – Buying Agency Agency () -
Vendor’s Account Number State Contract Number Purchase Order Number for Buying Agency 437001-M15-CFD0407
Date(s) Needed Start Time End Time (Estimated)
Address – Location (Building Name, Street Address, Room Number, City, State and Zip Code)
Address Instructions (provide specific instructions on how to get to the above address)
Requested Language American Sign Language (ASL) Albanian Chinese / Mandarin Khmer (Cambodian) Somali Arabic (simplified) Korean Spanish Bosnian Croatian Laotian Thai Burmese Farsi (Persian) Polish Vietnamese Chin French Russian Other, specify Chinese / Cantonese Hmong Serbian Karen Dialect Required Interpretation requires specialized skills (optional) Yes No CDI (ASL) Education Scientific
If yes, please identify dialect QMHI (ASL) Legal Wisconsin Court Certified SC:L(ASL) Medical
Other Instructions or Comments
Cost per hour Total Travel Time Total Mileage Estimate Vendor Invoice (under contract) (travel time allowed on (mileage allowed on assignments 4 Email to: assignments 4 days or less and days or less) may not exceed 2 hours total / miles Fax to: shift without prior approval of the agency) Mail to:
To be Completed by Vendor Vendor Authorization Accept Decline Person Authorizing:
DCF-F-2603-E (R. 10/2015) F-82074A – Health Services To be Completed by Buying Agency at Time of Service In-Person Interpreter Services (actual) Interpreter Start Time End Time Location Mileage Total Billable Time Name
Interpreter Start Time End Time Location Mileage Total Billable Time Name
Interpreter Start Time End Time Location Mileage Total Billable Time Name
Interpreter Start Time End Time Location Mileage Total Billable Time Name
Interpreter Start Time End Time Location Mileage Total Billable Time Name
The section below is used by DHS Only. Account Coding and Cost Information – For Buying Agency Use Only (Do not send to vendor. This section is to be completed by the buying agency after translation has been received and submitted along with the request to pay invoice.) Bureau / Program name(s) Office Name % Fund (5) Appr (5) Dept (10) Account (7) Program (5)* Operating Unit Project (15) Activity (15) (5)*
*These are mandatory fields for DHS facilities and institutes only. SIGNATU Date Signed RE – Program Supervisor or Designee
DCF-F-2603-E (R. 10/2015) Page 2 F-82074A – Health Services