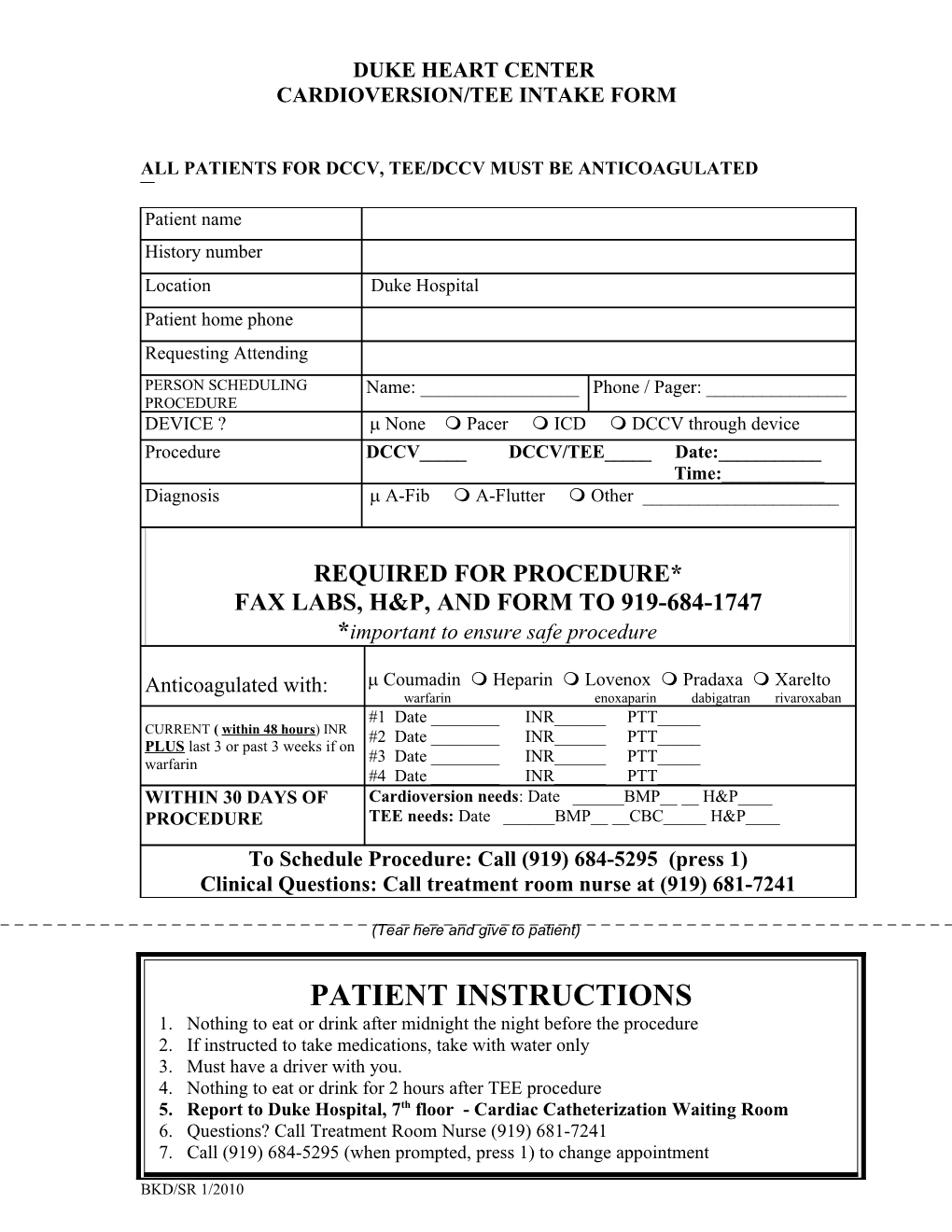
DUKE HEART CENTER CARDIOVERSION/TEE INTAKE FORM
ALL PATIENTS FOR DCCV, TEE/DCCV MUST BE ANTICOAGULATED
Patient name History number Location Duke Hospital Patient home phone Requesting Attending PERSON SCHEDULING Name: ______Phone / Pager: ______PROCEDURE DEVICE ? None Pacer ICD DCCV through device Procedure DCCV_____ DCCV/TEE_____ Date:______Time:______Diagnosis A-Fib A-Flutter Other ______
REQUIRED FOR PROCEDURE* FAX LABS, H&P, AND FORM TO 919-684-1747 *important to ensure safe procedure
Anticoagulated with: Coumadin Heparin Lovenox Pradaxa Xarelto warfarin enoxaparin dabigatran rivaroxaban #1 Date ______INR______PTT_____ CURRENT ( within 48 hours) INR #2 Date ______INR______PTT_____ PLUS last 3 or past 3 weeks if on warfarin #3 Date ______INR______PTT_____ #4 Date ______INR______PTT_____ WITHIN 30 DAYS OF Cardioversion needs: Date ______BMP__ __ H&P____ PROCEDURE TEE needs: Date ______BMP__ __CBC_____ H&P____ To Schedule Procedure: Call (919) 684-5295 (press 1) Clinical Questions: Call treatment room nurse at (919) 681-7241
(Tear here and give to patient)
PATIENT INSTRUCTIONS 1. Nothing to eat or drink after midnight the night before the procedure 2. If instructed to take medications, take with water only 3. Must have a driver with you. 4. Nothing to eat or drink for 2 hours after TEE procedure 5. Report to Duke Hospital, 7th floor - Cardiac Catheterization Waiting Room 6. Questions? Call Treatment Room Nurse (919) 681-7241 7. Call (919) 684-5295 (when prompted, press 1) to change appointment
BKD/SR 1/2010