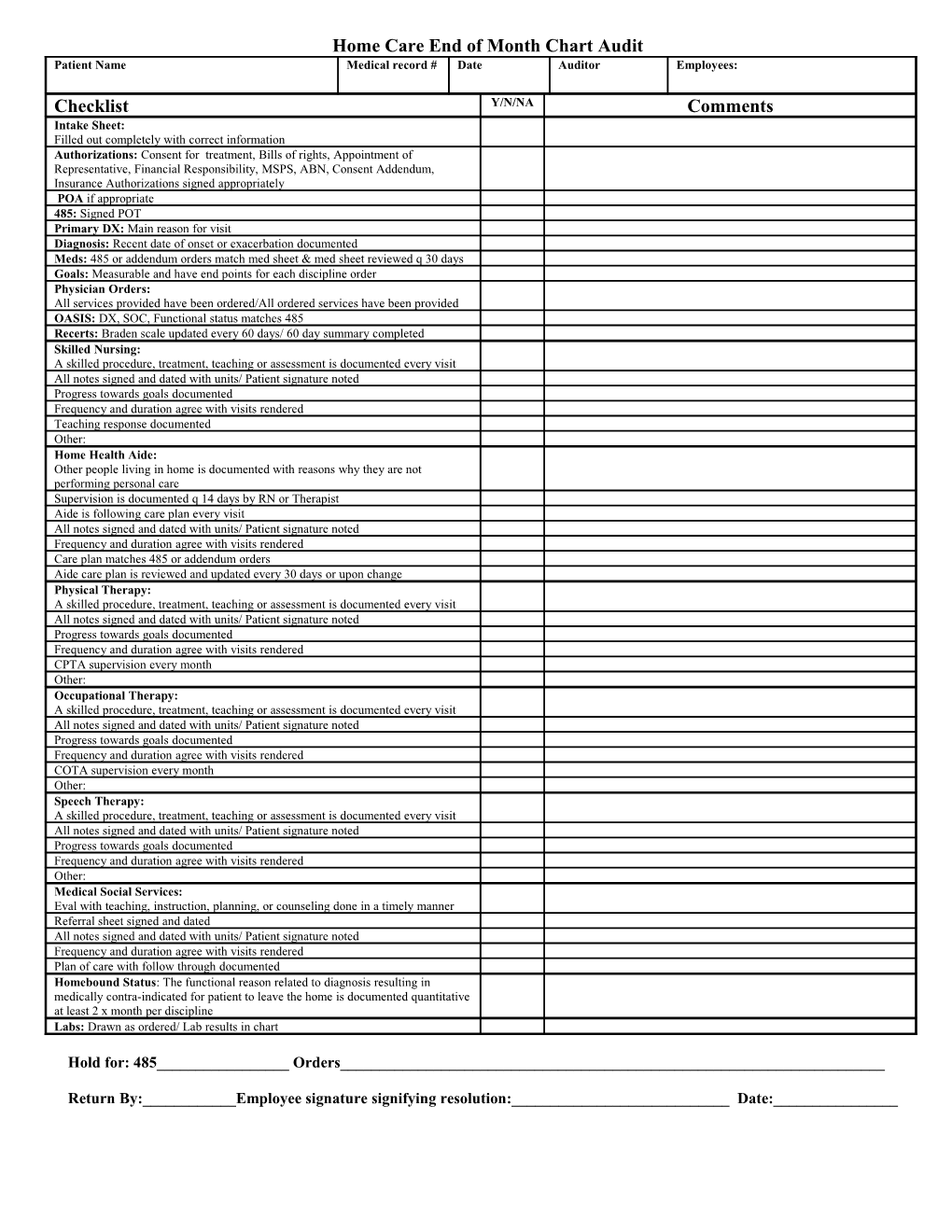
Home Care End of Month Chart Audit Patient Name Medical record # Date Auditor Employees:
Checklist Y/N/NA Comments Intake Sheet: Filled out completely with correct information Authorizations: Consent for treatment, Bills of rights, Appointment of Representative, Financial Responsibility, MSPS, ABN, Consent Addendum, Insurance Authorizations signed appropriately POA if appropriate 485: Signed POT Primary DX: Main reason for visit Diagnosis: Recent date of onset or exacerbation documented Meds: 485 or addendum orders match med sheet & med sheet reviewed q 30 days Goals: Measurable and have end points for each discipline order Physician Orders: All services provided have been ordered/All ordered services have been provided OASIS: DX, SOC, Functional status matches 485 Recerts: Braden scale updated every 60 days/ 60 day summary completed Skilled Nursing: A skilled procedure, treatment, teaching or assessment is documented every visit All notes signed and dated with units/ Patient signature noted Progress towards goals documented Frequency and duration agree with visits rendered Teaching response documented Other: Home Health Aide: Other people living in home is documented with reasons why they are not performing personal care Supervision is documented q 14 days by RN or Therapist Aide is following care plan every visit All notes signed and dated with units/ Patient signature noted Frequency and duration agree with visits rendered Care plan matches 485 or addendum orders Aide care plan is reviewed and updated every 30 days or upon change Physical Therapy: A skilled procedure, treatment, teaching or assessment is documented every visit All notes signed and dated with units/ Patient signature noted Progress towards goals documented Frequency and duration agree with visits rendered CPTA supervision every month Other: Occupational Therapy: A skilled procedure, treatment, teaching or assessment is documented every visit All notes signed and dated with units/ Patient signature noted Progress towards goals documented Frequency and duration agree with visits rendered COTA supervision every month Other: Speech Therapy: A skilled procedure, treatment, teaching or assessment is documented every visit All notes signed and dated with units/ Patient signature noted Progress towards goals documented Frequency and duration agree with visits rendered Other: Medical Social Services: Eval with teaching, instruction, planning, or counseling done in a timely manner Referral sheet signed and dated All notes signed and dated with units/ Patient signature noted Frequency and duration agree with visits rendered Plan of care with follow through documented Homebound Status: The functional reason related to diagnosis resulting in medically contra-indicated for patient to leave the home is documented quantitative at least 2 x month per discipline Labs: Drawn as ordered/ Lab results in chart
Hold for: 485______Orders______
Return By:______Employee signature signifying resolution:______Date:______