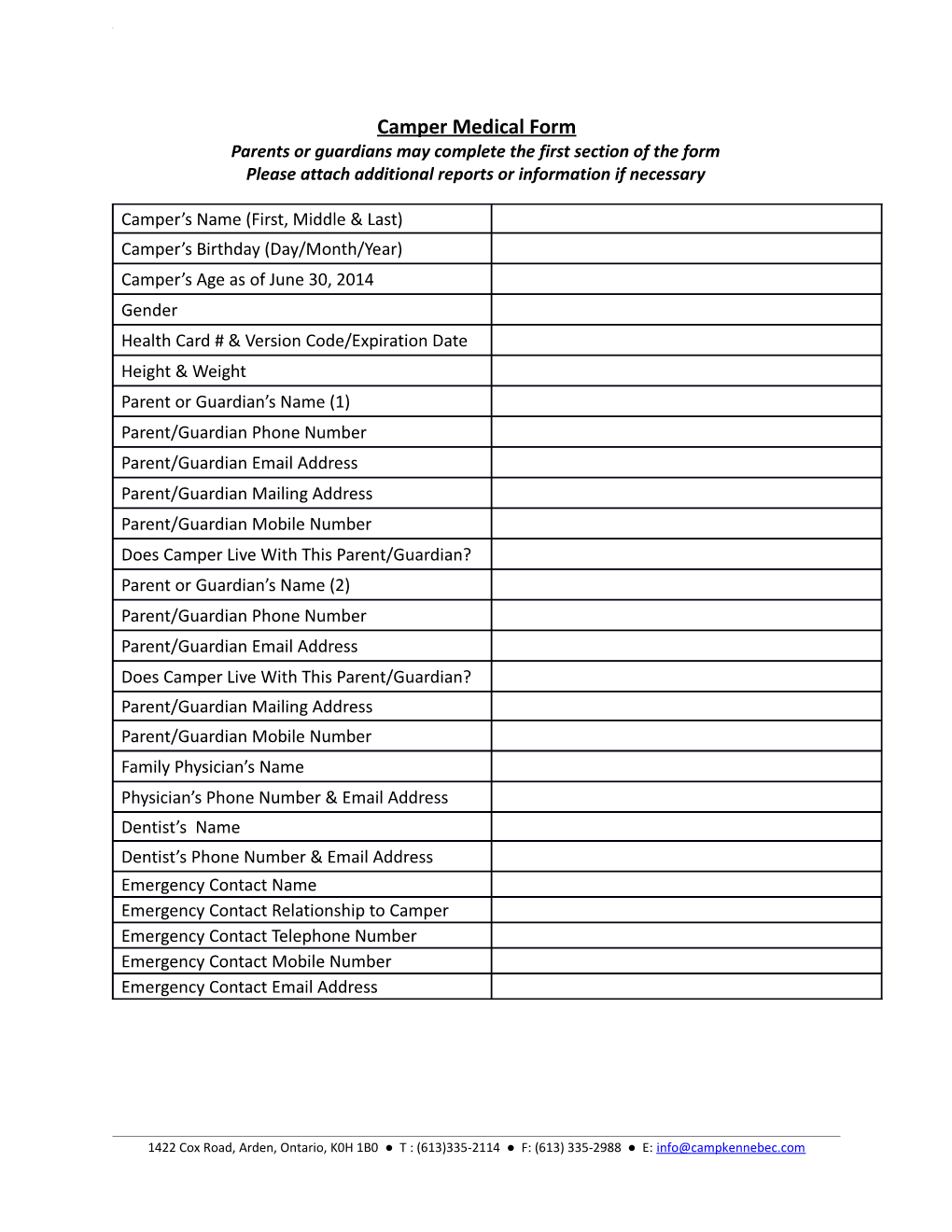
Camper Medical Form Parents or guardians may complete the first section of the form Please attach additional reports or information if necessary
Camper’s Name (First, Middle & Last) Camper’s Birthday (Day/Month/Year) Camper’s Age as of June 30, 2014 Gender Health Card # & Version Code/Expiration Date Height & Weight Parent or Guardian’s Name (1) Parent/Guardian Phone Number Parent/Guardian Email Address Parent/Guardian Mailing Address Parent/Guardian Mobile Number Does Camper Live With This Parent/Guardian? Parent or Guardian’s Name (2) Parent/Guardian Phone Number Parent/Guardian Email Address Does Camper Live With This Parent/Guardian? Parent/Guardian Mailing Address Parent/Guardian Mobile Number Family Physician’s Name Physician’s Phone Number & Email Address Dentist’s Name Dentist’s Phone Number & Email Address Emergency Contact Name Emergency Contact Relationship to Camper Emergency Contact Telephone Number Emergency Contact Mobile Number Emergency Contact Email Address
1422 Cox Road, Arden, Ontario, K0H 1B0 ● T : (613)335-2114 ● F: (613) 335-2988 ● E: [email protected] Camper Medical Form Physicians must complete the remainder of the form Please attach additional reports or information if necessary
1. Please list all camper medication, food or environmental allergies. Please describe potential reactions, especially those that may produce anaphylaxis or other serious medical issues. Also, include recommended treatment plans for reactions. ______
2. Has the camper had any injuries or illnesses within the past year? Does the treatment of these injuries or illnesses require special care or prevent full participation in the camp program? ______
3. Does a camper’s medical condition restrict participation in the camp program? Please list all relevant medical conditions and related restrictions in detail. ______
1422 Cox Road, Arden, Ontario, K0H 1B0 ● T : (613)335-2114 ● F: (613) 335-2988 ● E: [email protected] 4. Are all immunizations up-to-date? Please provide a listing of all immunizations and dates, including last tetanus shot. ______
5. Please list all current medications including dose, frequency including epi-pens, inhalers, PRN medications, vitamins & supplements. All medications must be blister-packed by pharmacist in the correct dose. How long has your child been stabilized on these medications?
Length of time camper has been Administration Time Medication Dosage stable on medication and any (Please Circle) additional notes Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
Wake Up Breakfast Lunch Dinner Bedtime Other
1422 Cox Road, Arden, Ontario, K0H 1B0 ● T : (613)335-2114 ● F: (613) 335-2988 ● E: [email protected] 6. Please circle the following Over the Counter (OTC) medications that camp can administer. We will follow the recommended dose on the consumer packaging, unless a physician advises Camp otherwise. Please do not send OTC medication to camp. We have these medications on site.
Tylenol Eye/Ear Drops Advil Cold & Sinus Medication Cough Syrup Imodium Gravol Benadryl Polysporin Throat Lozenges Cortisone Creams Calamine Lotion Pepto-Bismol Antihistamines (Reactine, Claritin)
Physician Statement
This health history is correct and complete to the best of my knowledge. The camper listed above has permission to participate in Camp Kennebec’s program subject to any restrictions noted above. To the best of my knowledge, this camper is in good health and has not had exposure to infectious diseases in the past four weeks. If I become aware that the camper has had exposure to an infectious disease prior to arrival at Camp Kennebec, I will notify Camp Kennebec immediately.
Physician Name: ______Physician Signature: ______Date: ______Phone #______Email: ______
The Ontario Camping Association standards for summer camps state that the camper’s physician must sign all medical forms. Please be advised that camp will not administer prescribed or over the counter medication without a physician-signed medical form.
Thank You
1422 Cox Road, Arden, Ontario, K0H 1B0 ● T : (613)335-2114 ● F: (613) 335-2988 ● E: [email protected]