Meridian World School - Medical and Insurance Information and Parent Consent for Student Travel and Medical Treatment
Student Name ______Home Address ______Phone ______Parent/Guardian ______Phone ______Parent/Guardian ______Phone ______
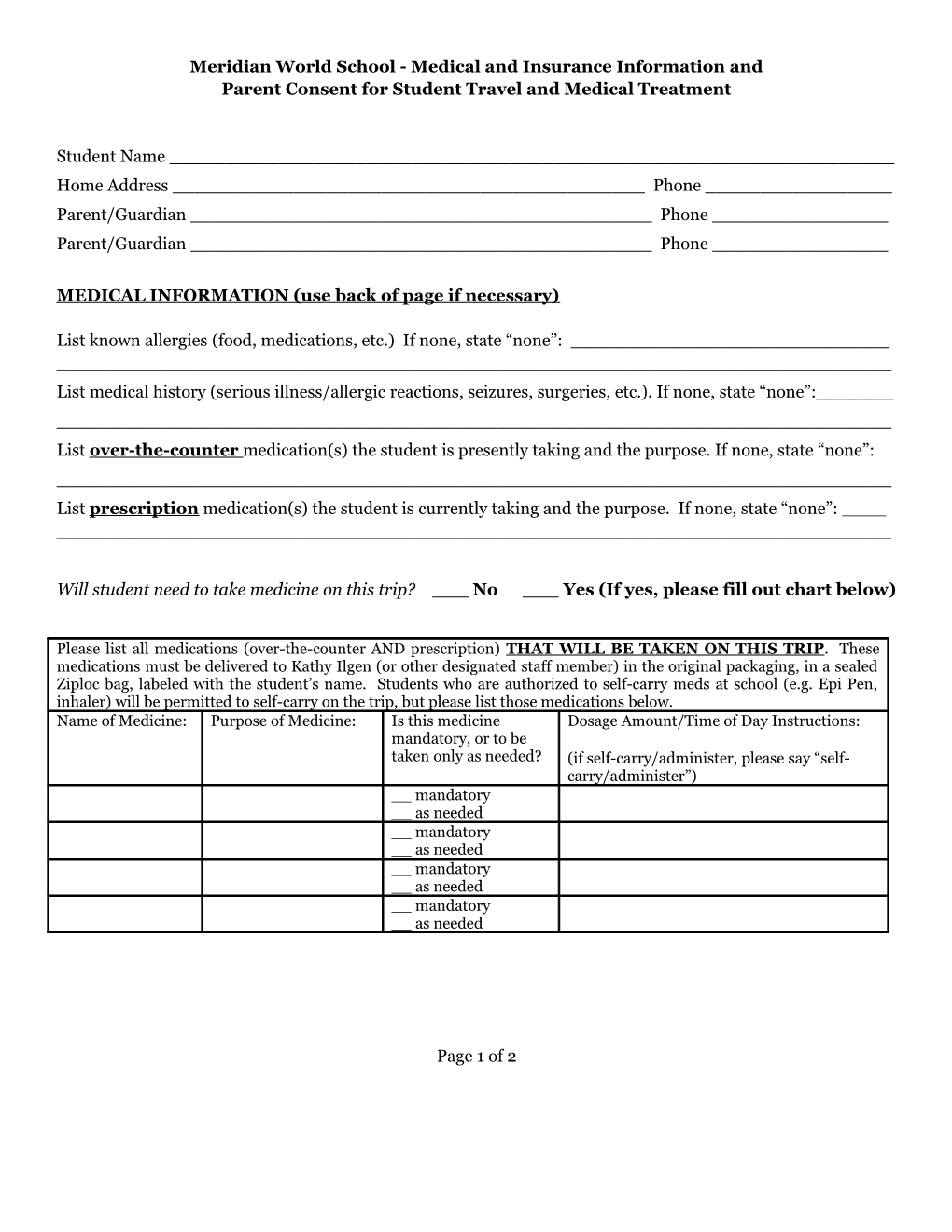
MEDICAL INFORMATION (use back of page if necessary)
List known allergies (food, medications, etc.) If none, state “none”: ______List medical history (serious illness/allergic reactions, seizures, surgeries, etc.). If none, state “none”:______List over-the-counter medication(s) the student is presently taking and the purpose. If none, state “none”: ______List prescription medication(s) the student is currently taking and the purpose. If none, state “none”: ______
Will student need to take medicine on this trip? ___ No ___ Yes (If yes, please fill out chart below)
Please list all medications (over-the-counter AND prescription) THAT WILL BE TAKEN ON THIS TRIP. These medications must be delivered to Kathy Ilgen (or other designated staff member) in the original packaging, in a sealed Ziploc bag, labeled with the student’s name. Students who are authorized to self-carry meds at school (e.g. Epi Pen, inhaler) will be permitted to self-carry on the trip, but please list those medications below. Name of Medicine: Purpose of Medicine: Is this medicine Dosage Amount/Time of Day Instructions: mandatory, or to be taken only as needed? (if self-carry/administer, please say “self- carry/administer”) __ mandatory __ as needed __ mandatory __ as needed __ mandatory __ as needed __ mandatory __ as needed
Page 1 of 2 MEDICAL INSURANCE INFORMATION
Medical Insurance Company ______Ins. Co. Phone #______Policy # ______Group/Plan # ______Current Physician ______Phone ______
____ Please check here to indicate that you have attached a copy of medical insurance identification card.
CONSENT FOR TRAVEL AND FOR MEDICAL TREATMENT
I, undersigned, being the parent or the legal guardian of ______, (Student Name) with date of birth ______, hereby grant permission for the above named student to travel to (MM/DD/Year)
Ecuador from March 11-18, 2017 and hereby grant authorization to Charles Ryder, Stela Holcombe and/or Mark Rogers to obtain any emergency medical and/or surgical treatment and procedures from a physician or hospital emergency room physician on behalf of the above named student, as well as grant permission to administer medication as indicated by physician.
______Printed Name of Person Giving Consent Signature
______Relationship to student Phone Number
Page 2 of 2