The University of Akron Employee and Student Office of the Associate Vice President/Controller Accounts Payable Direct Deposit Authorization
1. Please complete form and return to the Accounts Payable department with a canceled check which identifies both your account number and the depository’s (financial institution) nine-digit transit routing number.
2. The University of Akron will deposit payments directly into your bank account and send an e-mail notification of the deposit so that you know when the money is available to you.
3. Contact Accounts Payable with any questions at (330) 972-7200. Section 1: Depository Information
Depository (Bank) Name: Transit Routing Number: Account: Check only one: Checking Savings
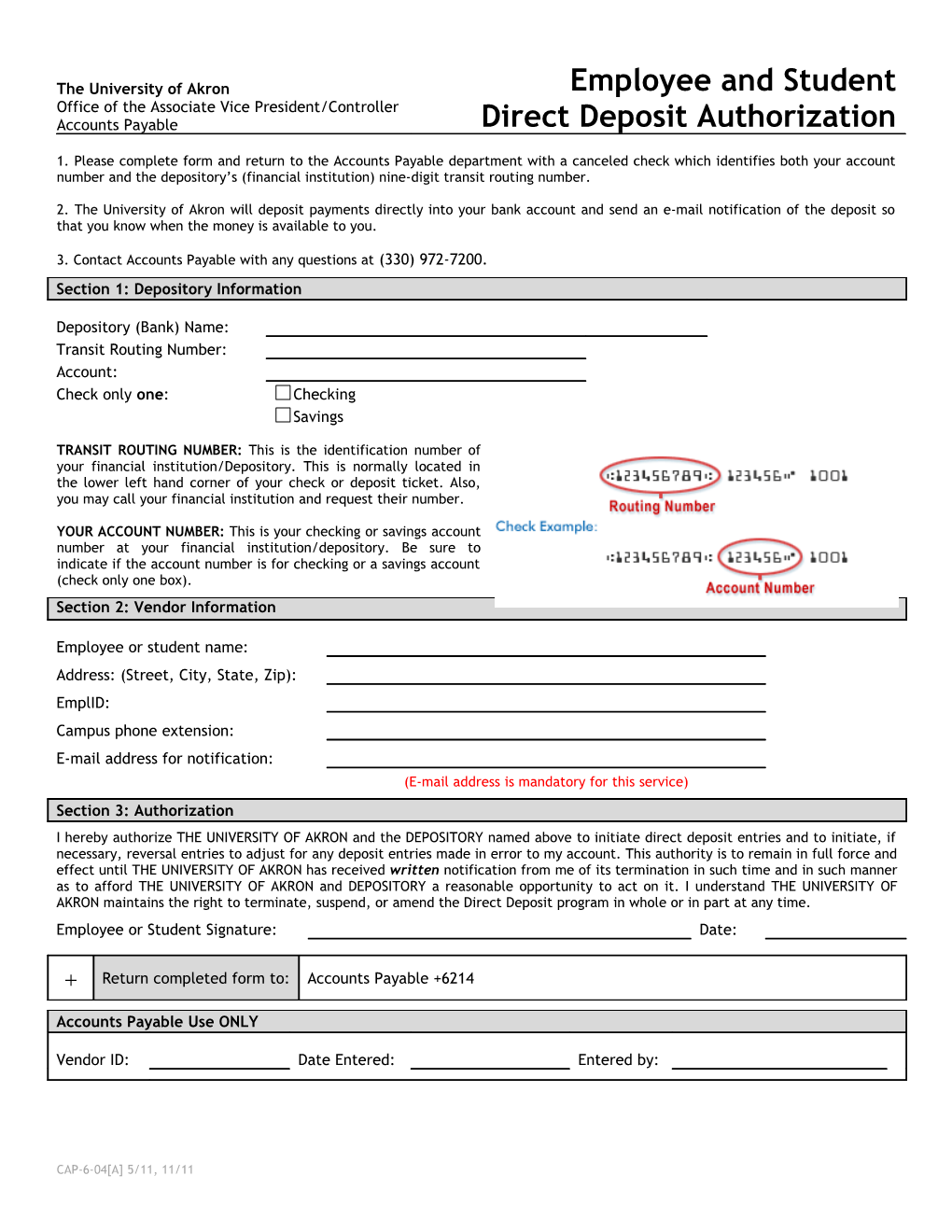
TRANSIT ROUTING NUMBER: This is the identification number of your financial institution/Depository. This is normally located in the lower left hand corner of your check or deposit ticket. Also, you may call your financial institution and request their number.
YOUR ACCOUNT NUMBER: This is your checking or savings account number at your financial institution/depository. Be sure to indicate if the account number is for checking or a savings account (check only one box). Section 2: Vendor Information
Employee or student name: Address: (Street, City, State, Zip): EmplID: Campus phone extension: E-mail address for notification: (E-mail address is mandatory for this service) Section 3: Authorization I hereby authorize THE UNIVERSITY OF AKRON and the DEPOSITORY named above to initiate direct deposit entries and to initiate, if necessary, reversal entries to adjust for any deposit entries made in error to my account. This authority is to remain in full force and effect until THE UNIVERSITY OF AKRON has received written notification from me of its termination in such time and in such manner as to afford THE UNIVERSITY OF AKRON and DEPOSITORY a reasonable opportunity to act on it. I understand THE UNIVERSITY OF AKRON maintains the right to terminate, suspend, or amend the Direct Deposit program in whole or in part at any time. Employee or Student Signature: Date:
Return completed form to: Accounts Payable +6214
Accounts Payable Use ONLY
Vendor ID: Date Entered: Entered by:
CAP-6-04[A] 5/11, 11/11