DRUG AND ALCOHOL TESTING CENTERS, INC. A Division of A.R.M. JUDGE DISTRICT COURT: CITY: PROBATION OFFICER: PHONE NUMBER (248) 305-6460 CHARGE: CASE NUMBER NAME: DOB: SEX: M F ADDRESS: PHONE NUMBER: CITY COMMENTS: STATE, ZIP: CHECK DESIRED TESTING: Alcohol Only ($5 per visit) Drugs Only Alcohol & Drugs Lab Analysis Oral $15 Urine $10 Oral $15 Urine $10 Oral $30 Urine $25 TESTING OPTION (Please Check below): X FREQUENCY (Please specify number of times weekly/monthly) DURATION OF TESTING (specify terms of testing) Daily Testing Random ( x week) Random ( x month) Weekends Only (Saturday & Sunday) HOLIDAY TESTING ONLY Other: Testing Start Date: Drug History / Last Date of Use:
Other Reporting Requirements / RX Meds being taken:
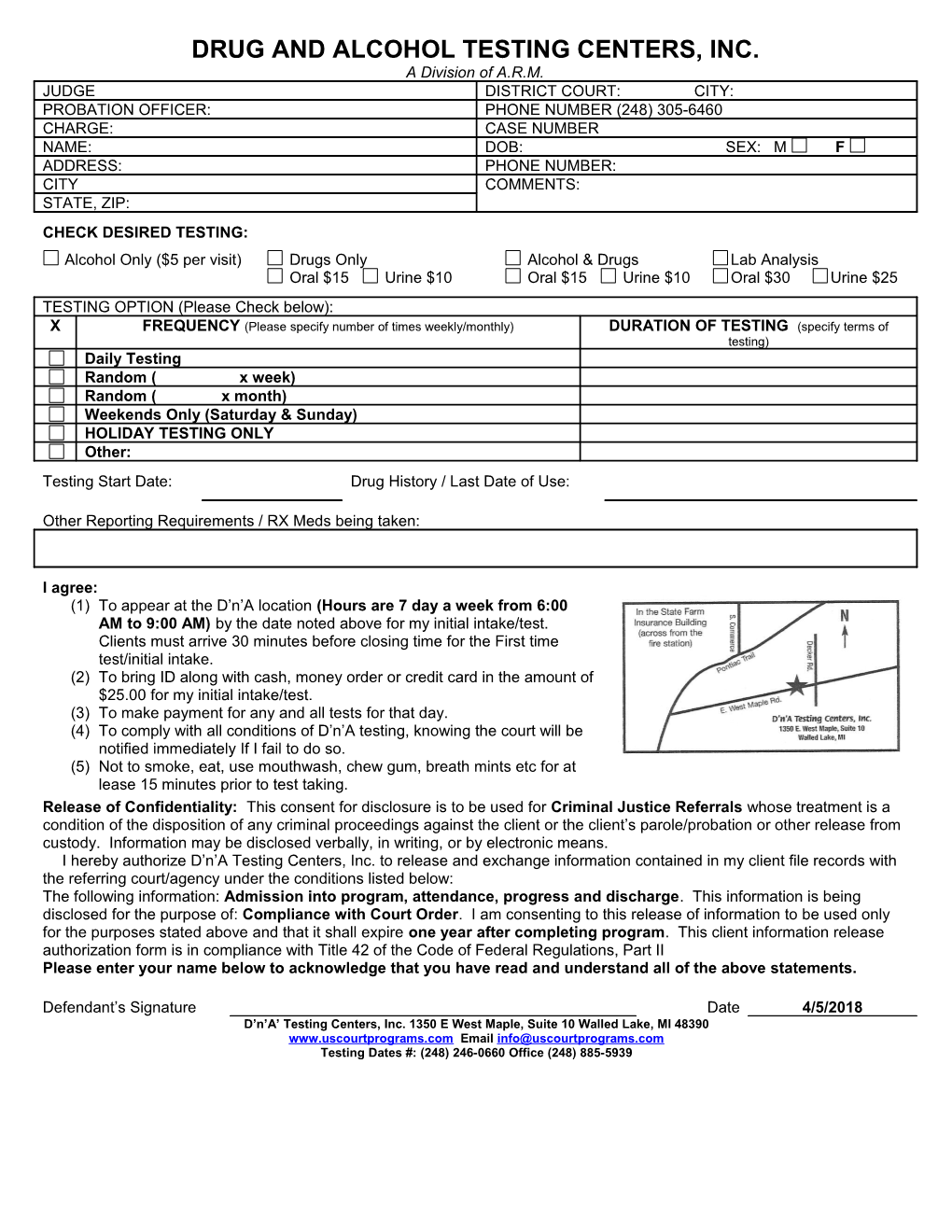
I agree: (1) To appear at the D’n’A location (Hours are 7 day a week from 6:00 AM to 9:00 AM) by the date noted above for my initial intake/test. Clients must arrive 30 minutes before closing time for the First time test/initial intake. (2) To bring ID along with cash, money order or credit card in the amount of $25.00 for my initial intake/test. (3) To make payment for any and all tests for that day. (4) To comply with all conditions of D’n’A testing, knowing the court will be notified immediately If I fail to do so. (5) Not to smoke, eat, use mouthwash, chew gum, breath mints etc for at lease 15 minutes prior to test taking. Release of Confidentiality: This consent for disclosure is to be used for Criminal Justice Referrals whose treatment is a condition of the disposition of any criminal proceedings against the client or the client’s parole/probation or other release from custody. Information may be disclosed verbally, in writing, or by electronic means. I hereby authorize D’n’A Testing Centers, Inc. to release and exchange information contained in my client file records with the referring court/agency under the conditions listed below: The following information: Admission into program, attendance, progress and discharge. This information is being disclosed for the purpose of: Compliance with Court Order. I am consenting to this release of information to be used only for the purposes stated above and that it shall expire one year after completing program. This client information release authorization form is in compliance with Title 42 of the Code of Federal Regulations, Part II Please enter your name below to acknowledge that you have read and understand all of the above statements.
Defendant’s Signature Date 4/5/2018 D’n’A’ Testing Centers, Inc. 1350 E West Maple, Suite 10 Walled Lake, MI 48390 www.uscourtprograms.com Email [email protected] Testing Dates #: (248) 246-0660 Office (248) 885-5939