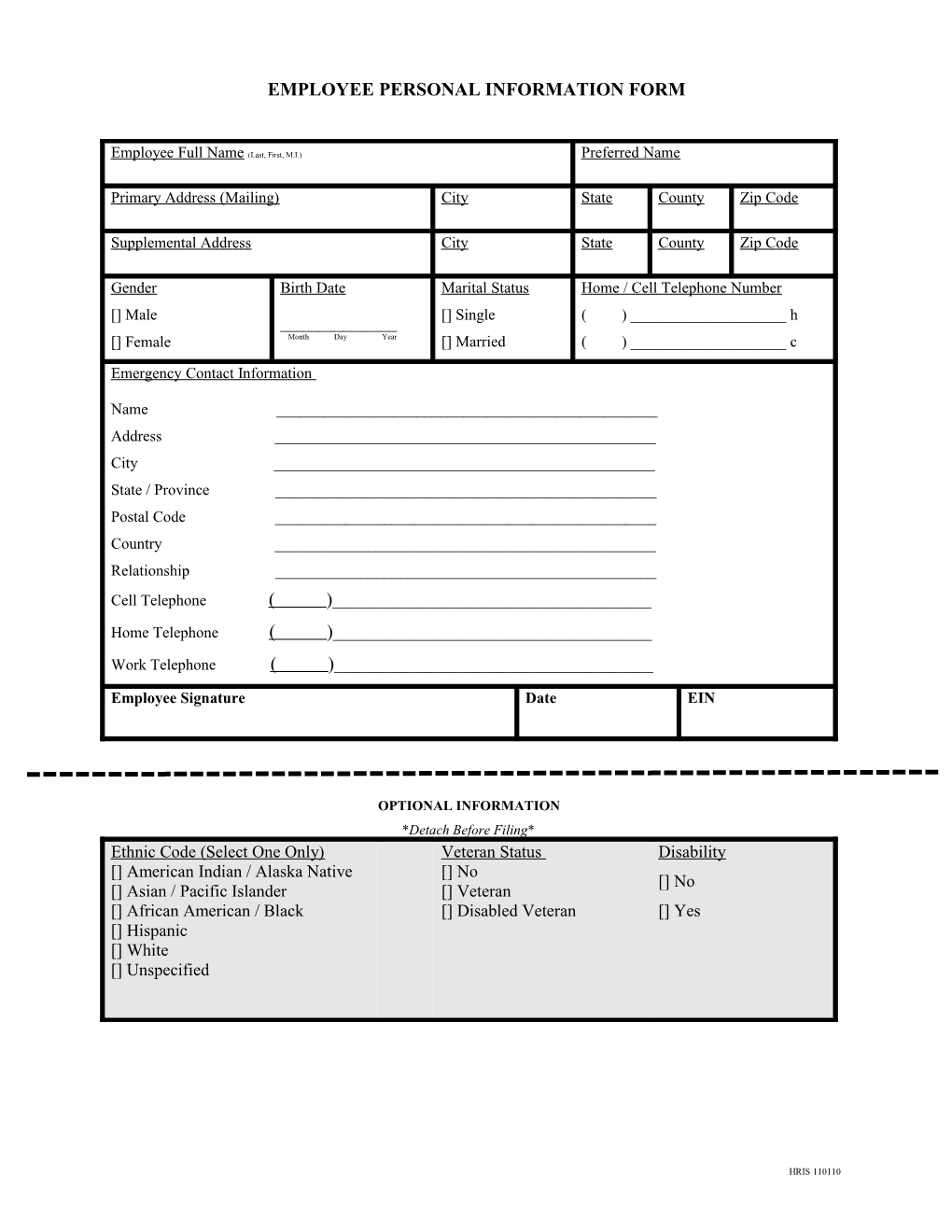
EMPLOYEE PERSONAL INFORMATION FORM
Employee Full Name (Last, First, M.I.) Preferred Name
Primary Address (Mailing) City State County Zip Code
Supplemental Address City State County Zip Code
Gender Birth Date Marital Status Home / Cell Telephone Number [] Male [] Single ( ) ______h ______[] Female Month Day Year [] Married ( ) ______c
Emergency Contact Information
Name ______Address ______City ______State / Province ______Postal Code ______Country ______Relationship ______Cell Telephone ( )______Home Telephone ( )______Work Telephone ( )______
Employee Signature Date EIN
OPTIONAL INFORMATION *Detach Before Filing* Ethnic Code (Select One Only) Veteran Status Disability [] American Indian / Alaska Native [] No [] No [] Asian / Pacific Islander [] Veteran [] African American / Black [] Disabled Veteran [] Yes [] Hispanic [] White [] Unspecified
HRIS 110110