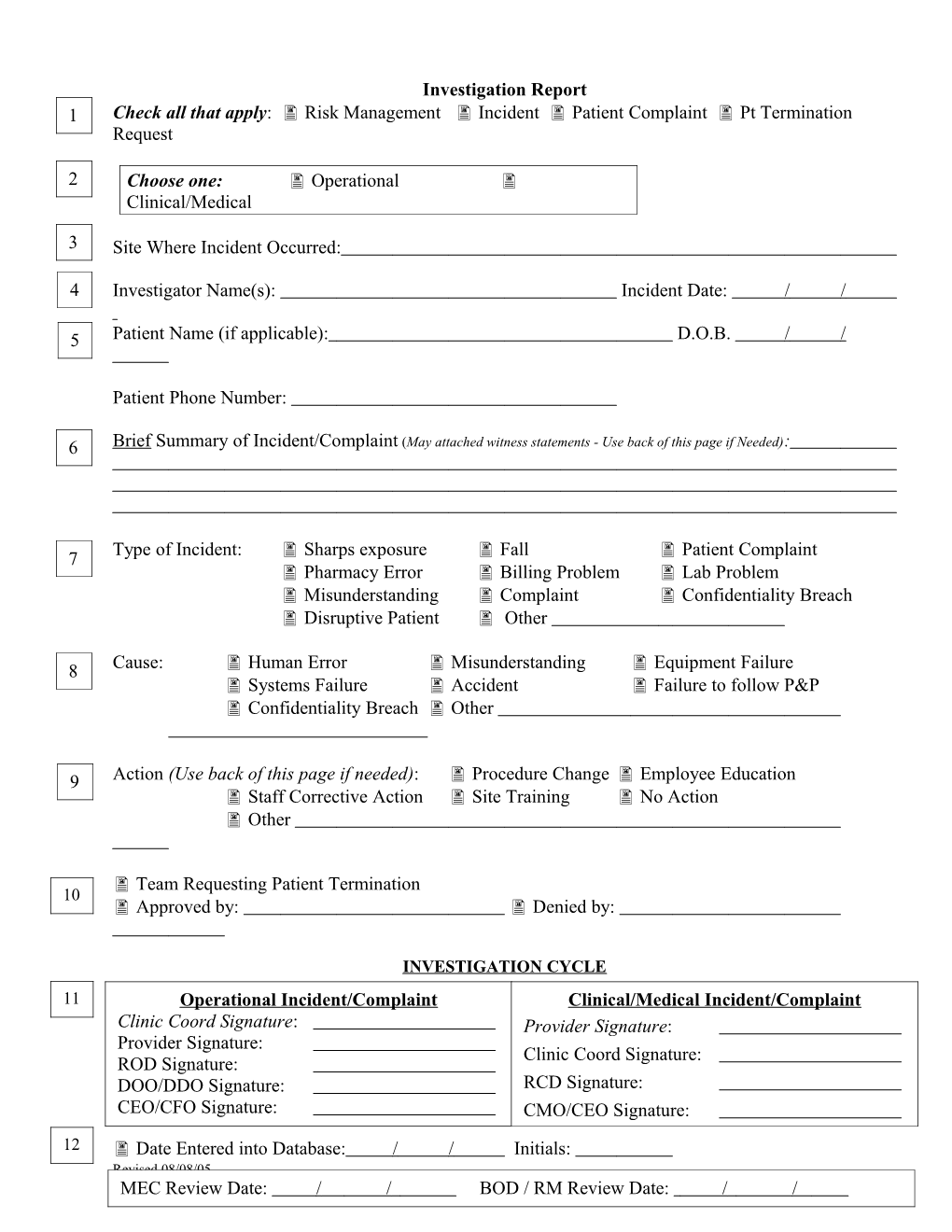
Investigation Report 1 Check all that apply: Risk Management Incident Patient Complaint Pt Termination . Request
2 Choose one: Operational . Clinical/Medical
3 Site Where Incident Occurred: . 4 Investigator Name(s): Incident Date: / / . 5 Patient Name (if applicable): D.O.B. / / . Patient Phone Number:
6 Brief Summary of Incident/Complaint (May attached witness statements - Use back of this page if Needed): .
Type of Incident: Sharps exposure Fall Patient Complaint 7 Pharmacy Error Billing Problem Lab Problem Misunderstanding Complaint Confidentiality Breach Disruptive Patient Other
8 Cause: Human Error Misunderstanding Equipment Failure . Systems Failure Accident Failure to follow P&P Confidentiality Breach Other
9 Action (Use back of this page if needed): Procedure Change Employee Education Staff Corrective Action Site Training No Action Other
Team Requesting Patient Termination 10 . Approved by: Denied by:
INVESTIGATION CYCLE 11 Operational Incident/Complaint Clinical/Medical Incident/Complaint Clinic Coord Signature: Provider Signature: Provider Signature: Clinic Coord Signature: ROD Signature: DOO/DDO Signature: RCD Signature: CEO/CFO Signature: CMO/CEO Signature:
12 Date Entered into Database: / / Initials: Revised 08/08/05 MEC Review Date: / / BOD / RM Review Date: / / 13
14 Case Closed – Initials Date / /
Revised 08/08/05