Version Date: 7/07/03
Patient Questionnaires:
1. DASH SCORE (Disabilities of the Arm, Shoulder and Hand) 2. American Shoulder and Elbow Score 3. SF-36
I. DASH SCORE
DISABILITIES OF THE ARM, SHOULDER, AND HAND SCORE
Patient Name: ______Date: ______
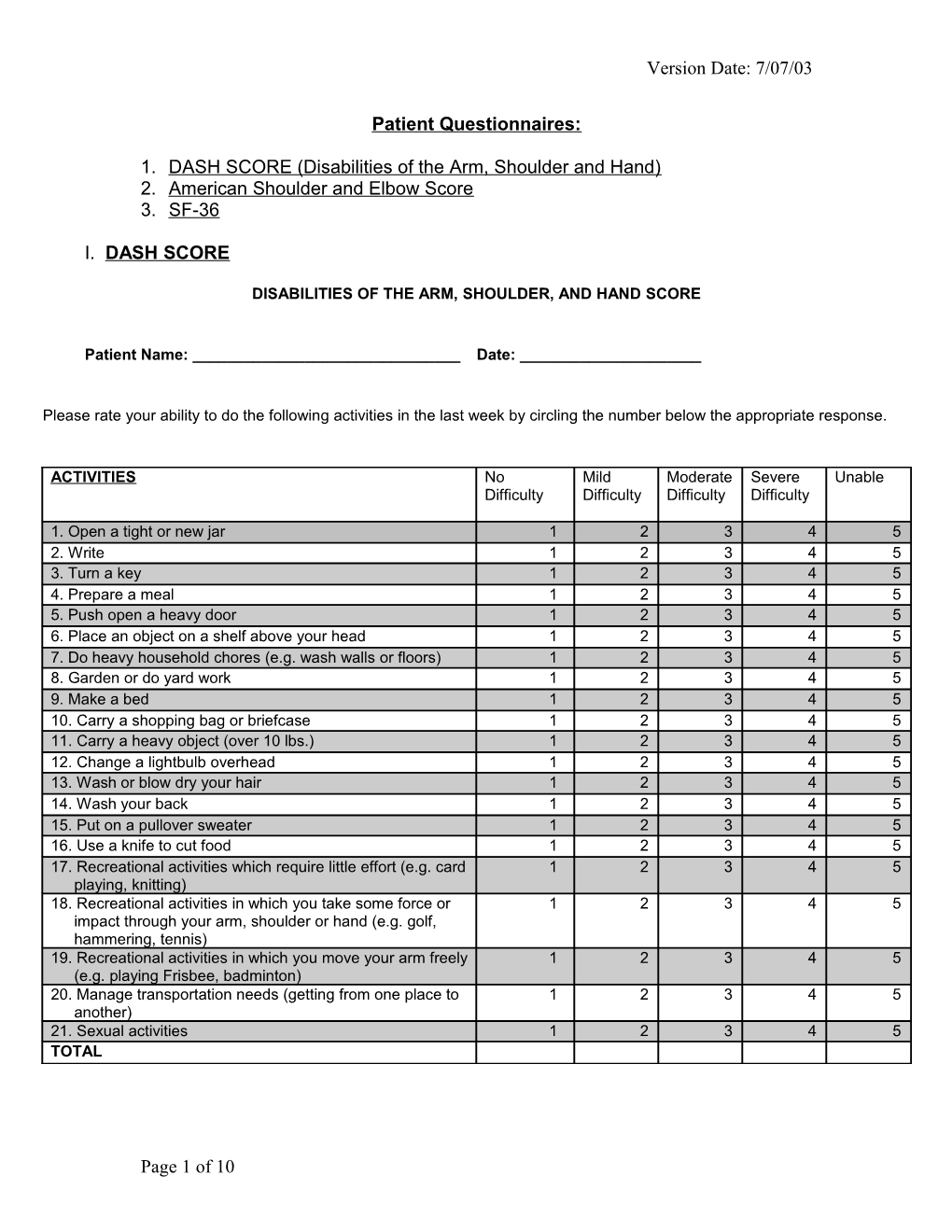
Please rate your ability to do the following activities in the last week by circling the number below the appropriate response.
ACTIVITIES No Mild Moderate Severe Unable Difficulty Difficulty Difficulty Difficulty
1. Open a tight or new jar 1 2 3 4 5 2. Write 1 2 3 4 5 3. Turn a key 1 2 3 4 5 4. Prepare a meal 1 2 3 4 5 5. Push open a heavy door 1 2 3 4 5 6. Place an object on a shelf above your head 1 2 3 4 5 7. Do heavy household chores (e.g. wash walls or floors) 1 2 3 4 5 8. Garden or do yard work 1 2 3 4 5 9. Make a bed 1 2 3 4 5 10. Carry a shopping bag or briefcase 1 2 3 4 5 11. Carry a heavy object (over 10 lbs.) 1 2 3 4 5 12. Change a lightbulb overhead 1 2 3 4 5 13. Wash or blow dry your hair 1 2 3 4 5 14. Wash your back 1 2 3 4 5 15. Put on a pullover sweater 1 2 3 4 5 16. Use a knife to cut food 1 2 3 4 5 17. Recreational activities which require little effort (e.g. card 1 2 3 4 5 playing, knitting) 18. Recreational activities in which you take some force or 1 2 3 4 5 impact through your arm, shoulder or hand (e.g. golf, hammering, tennis) 19. Recreational activities in which you move your arm freely 1 2 3 4 5 (e.g. playing Frisbee, badminton) 20. Manage transportation needs (getting from one place to 1 2 3 4 5 another) 21. Sexual activities 1 2 3 4 5 TOTAL
Page 1 of 10 Version Date: 7/07/03
DISABILITIES OF THE ARM, SHOULDER, AND HAND
Questions Not at all Slightly Moderately Quite a bit Extremely 22. During the past week, to what extent has your arm, shoulder or hand problem interfered with your normal social activities with family, friends, 1 2 3 4 5 neighbors or groups? (circle number)
Questions Not at all Slightly Moderately Quite a bit Extremely 23. During the past week, were you limited in your or other regular activities as a result of your arm, shoulder, or hand problem? (circle number) 1 2 3 4 5
Please rate the severity of the following symptoms in the last week. (Circle number) None Mild Moderate Severe Extreme 24. Arm, shoulder or hand pain. 1 2 3 4 5 25. Arm, shoulder or hand pain when you 1 2 3 4 5 performed any specific activity. 26. Tingling (pins and needles) in your arm, 1 2 3 4 5 shoulder or hand. 27. Weakness in your arm, shoulder or hand. 1 2 3 4 5 28. Stiffness in your arm, shoulder or hand. 1 2 3 4 5
Questions No Difficulty Mild Moderate Severe So Much Difficulty Difficulty Difficulty Difficulty I Can’t sleep 29. During the past week, how much difficulty have you had sleeping because of the pain in your arm, shoulder or hand? (circle number) 1 2 3 4 5
Questions Strongly Disagree Neither Agree Agree Strongly Disagree Nor Disagree Agree 30. I feel less capable, less confident or less useful because of my arm, shoulder or hand problem. (circle number) 1 2 3 4 5
TOTAL
FORMULA (RAW SCORE – 30) = DASH 12
Page 2 of 10 Version Date: 7/07/03
DISABILITIES OF THE ARM, SHOULDER AND HAND
Sports/Performing Arts Module (Optional)
The following questions relate to the impact of your arm, shoulder or hand problem on playing your musical instrument or sport or both. If you play more than one sport or instrument (or play both), please answer with respect to that activity which is most important to you. Please indicate the sport or instrument which is most important to you: ______
I do not play a sport or an instrument (You may skip this section).
Please circle the number that best describes your physical ability in the past week. Did you have any difficulty with:
ACTIVITIES No Difficulty Mild Moderate Severe Unable Difficulty Difficulty Difficulty 1. using your usual techniques for playing your 1 2 3 4 5 instrument or sport? 2. playing your musical instrument or sport because 1 2 3 4 5 of arm, shoulder or hand pain? 3. playing your musical instrument or sport as well 1 2 3 4 5 as you would like? 4. spending your usual amount of time practicing 1 2 3 4 5 or playing your instrument or sport? TOTAL
Work Module (Optional)
The following questions ask about the impact of your arm, shoulder or hand problem on your ability to work (including homemaking if that is your main work role). Please indicate what your job/work is: ______
I do not work (You may skip this section).
Please circle the number that best describes your physical ability in the past week. Did you have difficulty:
ACTIVITIES No Difficulty Mild Moderate Severe Unable Difficulty Difficulty Difficulty 1. using your usual techniques for work 1 2 3 4 5 2. doing your usual work because of arm, shoulder 1 2 3 4 5 or hand pain? 3. doing your work as well as you would like? 1 2 3 4 5 4. spending your usual amount of time doing your 1 2 3 4 5 work? TOTAL
FORMULA WORK/SPORTS: (RAW SCORE – 4) = DASH POTENTIAL
Page 3 of 10 Version Date: 7/07/03
II. American Shoulder and Elbow Score
0.16 SHOULDER ASSESSMENT FORM AMERICAN SHOULDER AND ELBOW SURGEONS
Name: Date:
Age: Hand dominance: R L Ambi Sex: M F
Diagnosis: Initial Assess? Y N
Procedure/Date: Follow-up: M Y
PATIENT SELF-EVALUATION Are you having pain in your shoulder? (circle correct answer) Yes No Mark where your pain is
Do you have pain in your shoulder at night? Yes No Do you take pain medication (aspirin, Advil, Tylenol, etc.)? Yes No Do you take narcotic pain medication (codeine or stronger)? Yes No How many pills do you take each day (average)? pills How bad is your pain today (mark line)? 0 10 No pain at all Pain as bad as it can be
Does your shoulder feel unstable (as if it is going to dislocate?) Yes No
How unstable is your shoulder (mark line)? 0 10 Very stable Very unstable
Page 4 of 10 Version Date: 7/07/03
Circle the number in the box that indicates your ability to do the following activities: 0 = Unable to do: 1 = Very difficult to do; 2 = Somewhat difficult; 3 = Not difficult ACTIVITY RIGHT ARM LEFT ARM 1. Put on a coat 0 1 2 3 0 1 2 3 2. Sleep on your painful or affected side 0 1 2 3 0 1 2 3 3. Wash back/do up bra in back 0 1 2 3 0 1 2 3 4. Manage toileting 0 1 2 3 0 1 2 3 5. Comb hair 0 1 2 3 0 1 2 3 6. Reach a high shelf 0 1 2 3 0 1 2 3 7. Lift 10 lbs. Above shoulder 0 1 2 3 0 1 2 3 8. Throw a ball overhand 0 1 2 3 0 1 2 3 9. Do usual work – List: 0 1 2 3 0 1 2 3 10. Do usual sport - List: 0 1 2 3 0 1 2 3
PHYSICIAN ASSESSMENT- to be performed by your doctor RANGE OF MOTION RIGHT LEFT Total shoulder motion Goniometer preferred Active Passive Active Passive
Forward elevation (Maximum arm-trunk angle)
External rotation (Arm comfortably at side)
External rotation (Arm at 90º abduction)
Internal rotation (Highest posterior anatomy reached with thumb)
Cross-body adduction (Antecubital fossa to opposite acromion)
SIGNS 0 = none; 1 = mild; 2 = moderate; 3 = severe SIGN Right Left Supraspinatus/greater tuberosity tenderness 0 1 2 3 0 1 2 3 AC joint tenderness 0 1 2 3 0 1 2 3 Biceps tendon tenderness 0 1 2 3 0 1 2 3 Other tenderness – List: 0 1 2 3 0 1 2 3
Impingement I (Passive forward elevation in alight internal rotation) Y N Y N
Impingement II (Passive internal rotation with 90º flexion) Y N Y N
Impingement III (90º active abduction - classic painful arc) Y N Y N Subacromial crepitus Y N Y N Scars – location: Y N Y N Atrophy – location: Y N Y N Deformity – describe: Y N Y N
Page 5 of 10 Version Date: 7/07/03
STRENGTH (record MRC grade)
0 = no contraction; 1 = flicker; 2 = movement with gravity eliminated; 3 = movement against gravity; 4 = movement against some resistance; 5 = normal power.
Right Left Testing affected by pain? Y N Y N Forward elevation 0 1 2 3 4 5 0 1 2 3 4 5 Abduction 0 1 2 3 4 5 0 1 2 3 4 5 External rotation (Arm comfortably at side) 0 1 2 3 4 5 0 1 2 3 4 5 Internal rotation (arm comfortably at side) 0 1 2 3 4 5 0 1 2 3 4 5
INSTABILITY 0 = none; 1 = mild( 0 – 1 cm translation); 2 = moderate (1 – 2 cm translation or translates to glenoid rim); 3 = severe (> 2 cm translation or over rim of glenoid)
Right Left Anterior translation 0 1 2 3 0 1 2 3 Posterior translation 0 1 2 3 0 1 2 3 Inferior translation (sulcus sign) 0 1 2 3 0 1 2 3 Anterior apprehension 0 1 2 3 0 1 2 3 Reduces symptoms? Y N Y N Voluntary instability? Y N Y N Relocation test positive? Y N Y N Generalized ligamentous laxity? Y N Y N Other physical findings:
Examiner’s name: Date:
Page 6 of 10 Version Date: 7/07/03
III. SF-36v2 Score
SF-36v2TM Health Survey Scoring Demonstration This survey asks for your views about your health. This information will help you keep track of how you feel and how well you are able to do your usual activities.
Answer every question by selecting the answer as indicated. If you are unsure about how to answer a question, please give the best answer you can.
1. In general, would you say your health is: [Click on the circle that best describes your answer.]
Excellent Very Good Good Fair Poor nmlkj nmlkj nmlkj nmlkj nmlkj
2. Compared to one year ago, how would you rate your health in general now?
Much better Somewhat better About the Somewhat worse Much worse now than one now than one same as one now than one now than one year ago year ago year ago year ago year ago nmlkj nmlkj nmlkj nmlkj nmlkj
3. The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much? [Click on a circle on each line.] Yes, Yes, No, not limited limited limited a lot a little at all a. Vigorous Activities, such as running, lifting heavy objects, participating in strenuous sports nmlkj nmlkj nmlkj
b. Moderate Activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf nmlkj nmlkj nmlkj
c. Lifting or carrying groceries nmlkj nmlkj nmlkj d. Climbing several flights of stairs nmlkj nmlkj nmlkj e. Climbing one flight of stairs nmlkj nmlkj nmlkj f. Bending, kneeling, or stooping nmlkj nmlkj nmlkj g. Walking more than a mile nmlkj nmlkj nmlkj h. Walking several hundred yards nmlkj nmlkj nmlkj i. Walking one hundred yards nmlkj nmlkj nmlkj j. Bathing or dressing yourself nmlkj nmlkj nmlkj
Page 7 of 10 Version Date: 7/07/03
4. During the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
A little All of Most of Some of None of of the time the time the time the time the time a. Cut down on the amount of time you spent on work or other activities nmlkj nmlkj nmlkj nmlkj nmlkj
b. Accomplished less than you would like nmlkj nmlkj nmlkj nmlkj nmlkj c. Were limited in the kind of work or other activities nmlkj nmlkj nmlkj nmlkj nmlkj d. Had difficulty performing the work or other activities (for nmlkj nmlkj nmlkj nmlkj nmlkj example, it took extra effort)
5. During the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)?
A little All of Most of Some of None of of the time the time the time the time the time a. Cut down on the amount of time you spent on work or other activities nmlkj nmlkj nmlkj nmlkj nmlkj
b. Accomplished less than you would like nmlkj nmlkj nmlkj nmlkj nmlkj c. Did work or activities less carefully than usual nmlkj nmlkj nmlkj nmlkj nmlkj
6. During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activities with family, friends, neighbors, or groups?
Not at all Slightly Moderately Quite a bit Extremely nmlkj nmlkj nmlkj nmlkj nmlkj
7. How much bodily pain have you had during the past 4 weeks?
None Very Mild Mild Moderate Severe Very Severe nmlkj nmlkj nmlkj nmlkj nmlkj nmlkj
8. During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?
Page 8 of 10 Version Date: 7/07/03
Not at all A little bit Moderately Quite a bit Extremely nmlkj nmlkj nmlkj nmlkj nmlkj
9. These questions are about how you feel and how things have been with you during the past 4 weeks. For each question, please give the one answer that comes closest to the way you have been feeling.
How much of the time during the past 4 weeks... A little All of Most of Some of None of of the time the time the time the time the time a. Did you feel full of life? nmlkj nmlkj nmlkj nmlkj nmlkj b. Have you been very nervous? nmlkj nmlkj nmlkj nmlkj nmlkj c. Have you felt so down in the dumps that nothing could cheer you up? nmlkj nmlkj nmlkj nmlkj nmlkj
d. Have you felt calm and peaceful? nmlkj nmlkj nmlkj nmlkj nmlkj e. Did you have a lot of energy? nmlkj nmlkj nmlkj nmlkj nmlkj f. Have you felt downhearted and depressed? nmlkj nmlkj nmlkj nmlkj nmlkj g. Did you feel worn out? nmlkj nmlkj nmlkj nmlkj nmlkj h. Have you been happy? nmlkj nmlkj nmlkj nmlkj nmlkj i. Did you feel tired? nmlkj nmlkj nmlkj nmlkj nmlkj
10. During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting friends, relatives, etc.)?
All of Most of Some of A little of None of the time the time the time the time the time nmlkj nmlkj nmlkj nmlkj nmlkj
11. How TRUE or FALSE is each of the following statements for you?
Definitely Mostly Don't Mostly Definitely true true Know false false a. I seem to get sick a little easier than other people nmlkj nmlkj nmlkj nmlkj nmlkj
b. I am as healthy as anybody I know nmlkj nmlkj nmlkj nmlkj nmlkj c. I expect my health to get worse nmlkj nmlkj nmlkj nmlkj nmlkj d. My health is excellent nmlkj nmlkj nmlkj nmlkj nmlkj
Page 9 of 10 Version Date: 7/07/03
Page 10 of 10