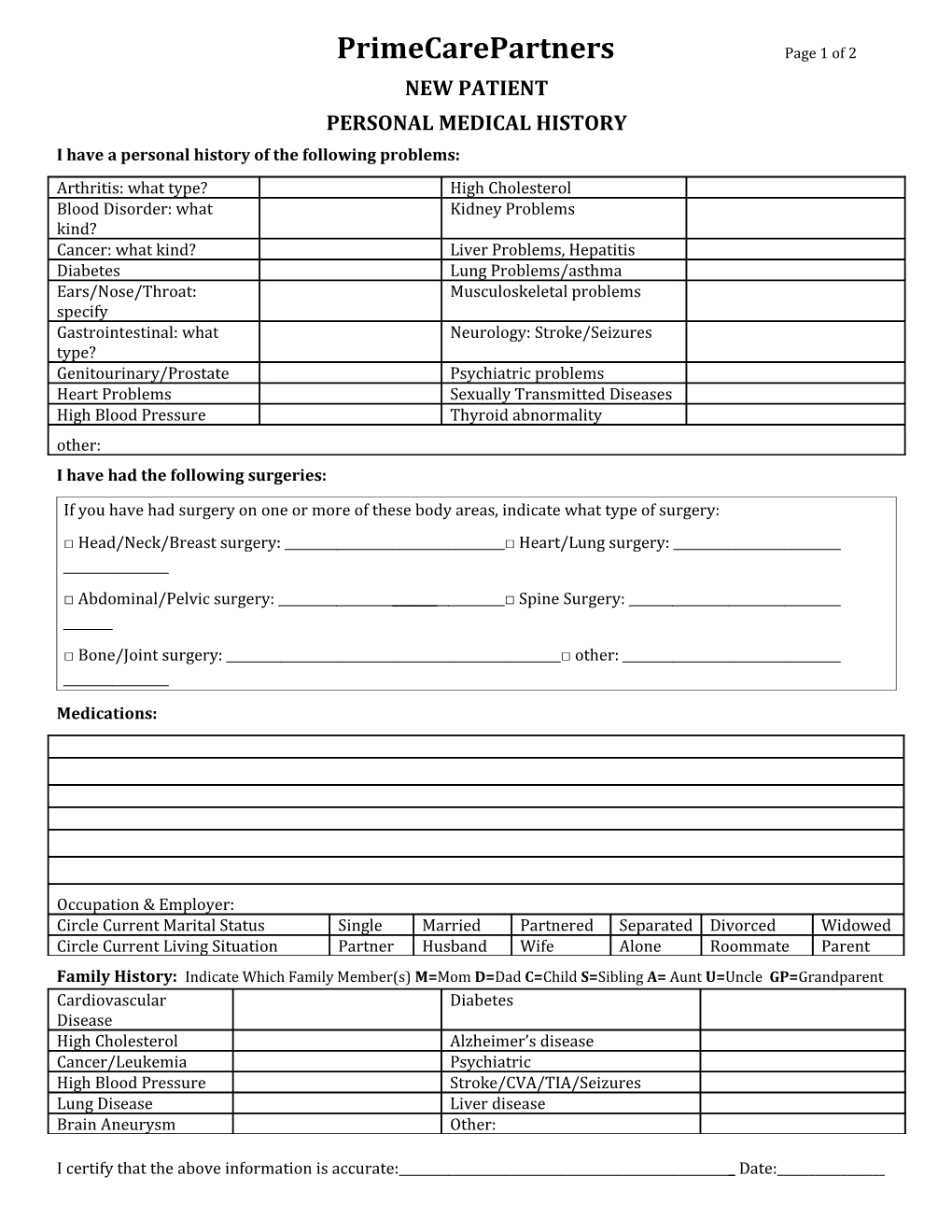
PrimeCarePartners Page 1 of 2 NEW PATIENT PERSONAL MEDICAL HISTORY I have a personal history of the following problems: Arthritis: what type? High Cholesterol Blood Disorder: what Kidney Problems kind? Cancer: what kind? Liver Problems, Hepatitis Diabetes Lung Problems/asthma Ears/Nose/Throat: Musculoskeletal problems specify Gastrointestinal: what Neurology: Stroke/Seizures type? Genitourinary/Prostate Psychiatric problems Heart Problems Sexually Transmitted Diseases High Blood Pressure Thyroid abnormality other: I have had the following surgeries:
If you have had surgery on one or more of these body areas, indicate what type of surgery: □ Head/Neck/Breast surgery: □ Heart/Lung surgery:
□ Abdominal/Pelvic surgery: ______□ Spine Surgery:
□ Bone/Joint surgery: □ other:
Medications:
Occupation & Employer: Circle Current Marital Status Single Married Partnered Separated Divorced Widowed Circle Current Living Situation Partner Husband Wife Alone Roommate Parent Family History: Indicate Which Family Member(s) M=Mom D=Dad C=Child S=Sibling A= Aunt U=Uncle GP=Grandparent Cardiovascular Diabetes Disease High Cholesterol Alzheimer’s disease Cancer/Leukemia Psychiatric High Blood Pressure Stroke/CVA/TIA/Seizures Lung Disease Liver disease Brain Aneurysm Other:
I certify that the above information is accurate: _ Date:______Patient’s signature (or patient’s representative) PCP New Patient Med history, Rev. 11/2013
Please See Backside → Page 2 of 2
I have had the following procedures: Test Date or Year Results (normal/abnormal) Colonoscopy Hemoccult (test for blood in stool) Mammogram DEXA (bone density test for osteoporosis) Cholesterol blood test Diabetes blood test Men only: PSA (prostate blood test) Men only: AAA screen (abdominal aorta ultrasound) Women only: Pap smear
I have had the following Vaccines: Vaccine Date/Year Administered Tetanus Pertussis Influenza (flu) Pneumonia Hepatitis A Hepatitis B Meningitis HPV shingles
These are the specialists currently involved in my care (if any): Opthalmologist:______Cardiologist:______Pulmonologist:______Dermatologist:______Oncologist:______Orthopedist:______Ear/Nose/Throat:______Urologist:______Neurologist:______Gynecologist:______Gastroenterologist:______
For Women only: Have you ever had an abnormal Pap smear? Yes_____ No_____ If so, when and what (if any) procedures were done? ______Have you ever had an abnormal mammogram? Yes_____ No_____ If so, when and what (if any) procedures were done?______Have you had a hysterectomy? Yes_____ No_____ If so, what was the reason?______Are you still menstruating? Yes_____ No_____ If no, how old were you when you stopped?______I certify that the above information is accurate: ______Date:______Patient’s signature (or patient’s representative) PCP New Patient Med history, Rev. 11/2013