BEE ALLERGY ACTION PLAN
Student’s Name: ______D.O.B: ______Building: ______
ALLERGY TO: ______Asthma: Yes (higher risk for severe reaction) No
TREATMENT
Symptoms Give Circled Medication (to be determined by physician)
Child has been stung , but NO SYMPTOMS: Epinephrine Antihistamine Mouth: Itching, tingling, swelling of lips, tongue, mouth Epinephrine Antihistamine Skin: Hives, itchy rash, swelling of face or extremities Epinephrine Antihistamine Gut: Nausea, vomiting, cramps, diarrhea Epinephrine Antihistamine Throat: Tightening of throat, hoarseness, cough Epinephrine Antihistamine Heart: Thready pulse, fainting, pale, blueness Epinephrine Antihistamine Other: ______Epinephrine Antihistamine
Medication/Doses : Epinephrine (brand and dose):______
Antihistamine (brand and dose): ______
MD Signature: ______
Any Severe Symptoms after suspected sting INJECT EPINEPHRINE IMMEDIATELY and CALL 911
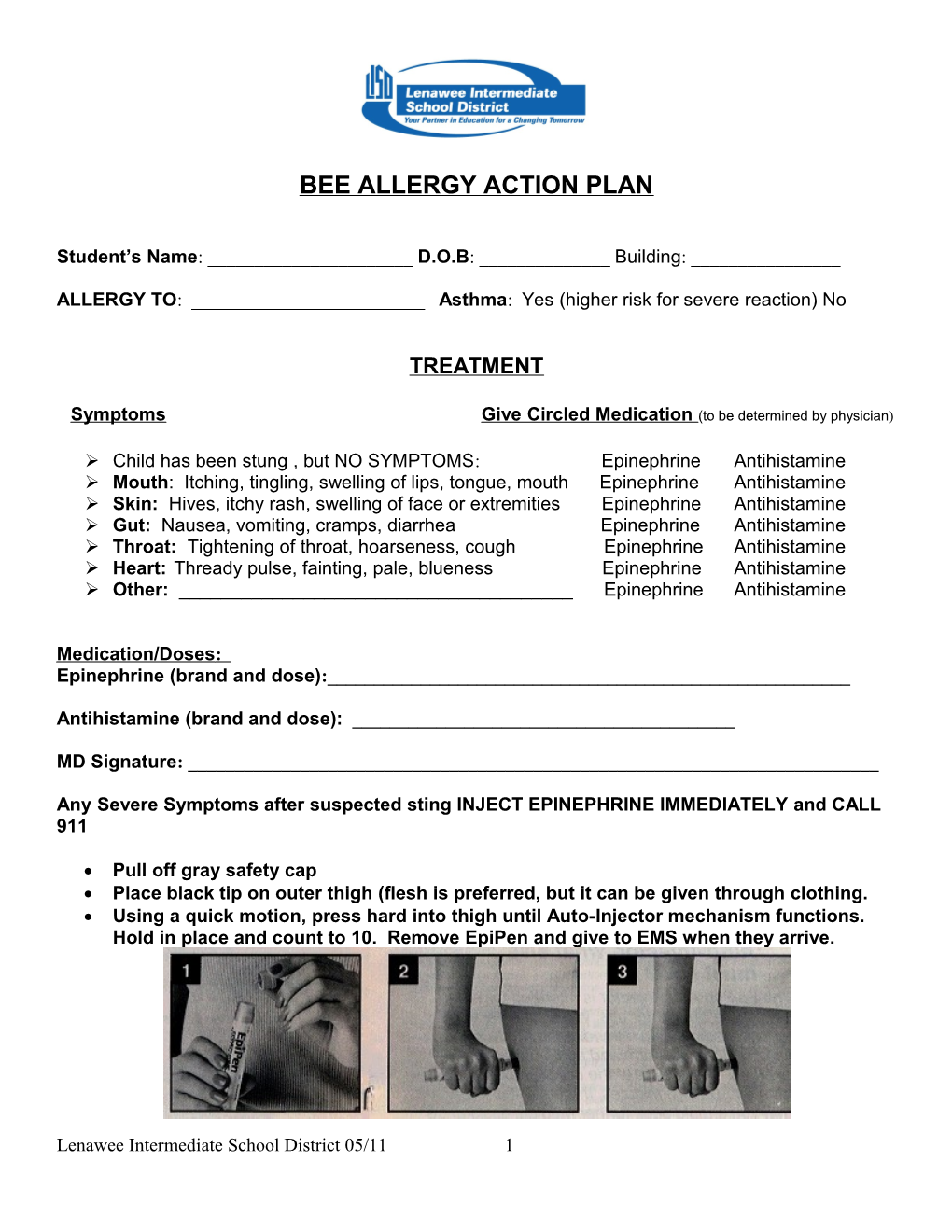
Pull off gray safety cap Place black tip on outer thigh (flesh is preferred, but it can be given through clothing. Using a quick motion, press hard into thigh until Auto-Injector mechanism functions. Hold in place and count to 10. Remove EpiPen and give to EMS when they arrive.
Lenawee Intermediate School District 05/11 1