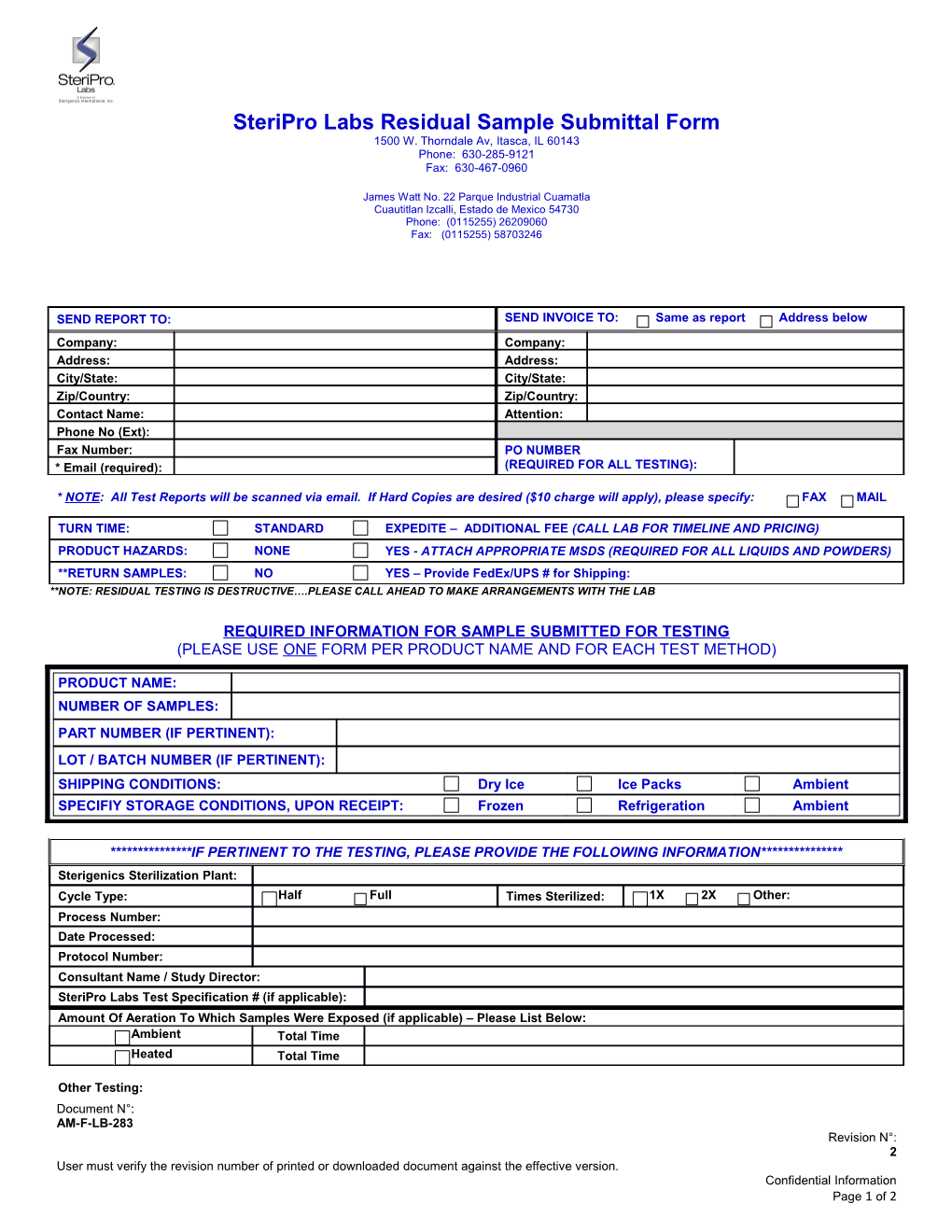
SteriPro Labs Residual Sample Submittal Form 1500 W. Thorndale Av, Itasca, IL 60143 Phone: 630-285-9121 Fax: 630-467-0960
James Watt No. 22 Parque Industrial Cuamatla Cuautitlan Izcalli, Estado de Mexico 54730 Phone: (0115255) 26209060 Fax: (0115255) 58703246
SEND REPORT TO: SEND INVOICE TO: Same as report Address below Company: Company: Address: Address: City/State: City/State: Zip/Country: Zip/Country: Contact Name: Attention: Phone No (Ext): Fax Number: PO NUMBER * Email (required): (REQUIRED FOR ALL TESTING):
* NOTE: All Test Reports will be scanned via email. If Hard Copies are desired ($10 charge will apply), please specify: FAX MAIL
TURN TIME: STANDARD EXPEDITE – ADDITIONAL FEE (CALL LAB FOR TIMELINE AND PRICING) PRODUCT HAZARDS: NONE YES - ATTACH APPROPRIATE MSDS (REQUIRED FOR ALL LIQUIDS AND POWDERS) **RETURN SAMPLES: NO YES – Provide FedEx/UPS # for Shipping: **NOTE: RESIDUAL TESTING IS DESTRUCTIVE….PLEASE CALL AHEAD TO MAKE ARRANGEMENTS WITH THE LAB
REQUIRED INFORMATION FOR SAMPLE SUBMITTED FOR TESTING (PLEASE USE ONE FORM PER PRODUCT NAME AND FOR EACH TEST METHOD)
PRODUCT NAME: NUMBER OF SAMPLES: PART NUMBER (IF PERTINENT): LOT / BATCH NUMBER (IF PERTINENT): SHIPPING CONDITIONS: Dry Ice Ice Packs Ambient SPECIFIY STORAGE CONDITIONS, UPON RECEIPT: Frozen Refrigeration Ambient
***************IF PERTINENT TO THE TESTING, PLEASE PROVIDE THE FOLLOWING INFORMATION*************** Sterigenics Sterilization Plant: Cycle Type: Half Full Times Sterilized: 1X 2X Other: Process Number: Date Processed: Protocol Number: Consultant Name / Study Director: SteriPro Labs Test Specification # (if applicable): Amount Of Aeration To Which Samples Were Exposed (if applicable) – Please List Below: Ambient Total Time Heated Total Time
Other Testing: Document N°: AM-F-LB-283 Revision N°: 2 User must verify the revision number of printed or downloaded document against the effective version. Confidential Information Page 1 of 2
SteriPro Labs Residual Sample Submittal Form 1500 W. Thorndale Av, Itasca, IL 60143 Phone: 630-285-9121 Fax: 630-467-0960
James Watt No. 22 Parque Industrial Cuamatla Cuautitlan Izcalli, Estado de Mexico 54730 Phone: (0115255) 26209060 Fax: (0115255) 58703246
EXOTHERMIC TESTING – ITASCA ONLY FOR STERIPRO LAB USE ONLY
# of Samples Received: ______Samples received on: Dry Ice Ice Packs Ambient
Verified By/Date:______Customer #: WO#: SO#:
Comments and/or Special Instructions:
Customer Signature: ______Date: ______(REQUIRED for Testing)
Document N°: AM-F-LB-283 Revision N°: 2 User must verify the revision number of printed or downloaded document against the effective version. Confidential Information Page 2 of 2