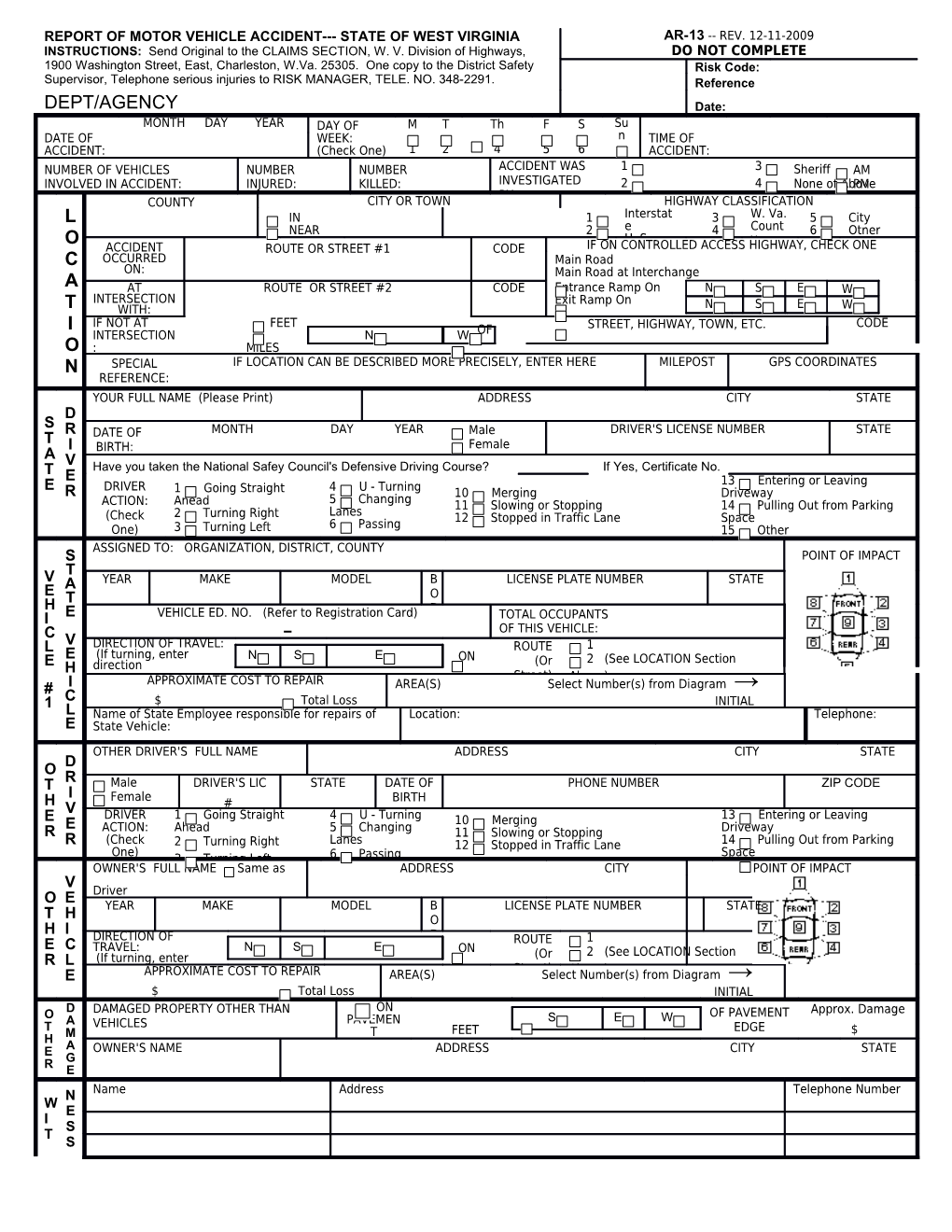
REPORT OF MOTOR VEHICLE ACCIDENT--- STATE OF WEST VIRGINIA AR-13 -- REV. 12-11-2009 INSTRUCTIONS: Send Original to the CLAIMS SECTION, W. V. Division of Highways, DO NOT COMPLETE 1900 Washington Street, East, Charleston, W.Va. 25305. One copy to the District Safety Risk Code: Supervisor, Telephone serious injuries to RISK MANAGER, TELE. NO. 348-2291. Reference DEPT/AGENCY Date: NAME MONTH DAY YEAR DAY OF M T Th F S Su DATE OF WEEK: n TIME OF ACCIDENT: (Check One) 1 2 4 5 6 ACCIDENT: 7 NUMBER OF VEHICLES NUMBER NUMBER ACCIDENT WAS 1 3 Sheriff AM INVOLVED IN ACCIDENT: INJURED: KILLED: INVESTIGATED 2 4 None of Above PM BY: COUNTY CITY OR TOWN HIGHWAY CLASSIFICATION L IN 1 Interstat 3 W. Va. 5 City NEAR 2 e 4 Count 6 Otner O U. S. y ACCIDENT ROUTE OR STREET #1 CODE IF ON CONTROLLED ACCESS HIGHWAY, CHECK ONE C OCCURRED Main Road ON: Main Road at Interchange A AT ROUTE OR STREET #2 CODE Entrance Ramp On N S E W INTERSECTION Exit Ramp On T WITH: N S E W I IF NOT AT FEET STREET, HIGHWAY, TOWN, ETC. CODE INTERSECTION N W OF O : MILES N SPECIAL IF LOCATION CAN BE DESCRIBED MORE PRECISELY, ENTER HERE MILEPOST GPS COORDINATES REFERENCE: YOUR FULL NAME (Please Print) ADDRESS CITY STATE D S R DATE OF MONTH DAY YEAR Male DRIVER'S LICENSE NUMBER STATE T I Female A BIRTH: V Have you taken the National Safey Council's Defensive Driving Course? If Yes, Certificate No. T E E DRIVER 13 Entering or Leaving R 1 Going Straight 4 U - Turning 10 Merging Driveway ACTION: Anead 5 Changing 11 Slowing or Stopping 14 Pulling Out from Parking (Check 2 Turning Right Lanes 12 Stopped in Traffic Lane Space One) 3 Turning Left 6 Passing 15 Other ASSIGNED TO: ORGANIZATION, DISTRICT, COUNTY S POINT OF IMPACT T V A YEAR MAKE MODEL B LICENSE PLATE NUMBER STATE E T O H D I E VEHICLE ED. NO. (Refer to Registration Card) TOTAL OCCUPANTS C - OF THIS VEHICLE: L V DIRECTION OF TRAVEL: ROUTE 1 E (If turning, enter N S E ON 2 (See LOCATION Section E H direction (Or BEFORE turn.)APPROXIMATE COST TO REPAIR Street) Above) # I AREA(S) Select Number(s) from Diagram → 1 C $ Total Loss INITIAL L Name of State Employee responsible for repairs of Location: Telephone: E State Vehicle:
OTHER DRIVER'S FULL NAME ADDRESS CITY STATE D O T R Male DRIVER'S LIC STATE DATE OF PHONE NUMBER ZIP CODE I Female H # BIRTH V DRIVER 1 Going Straight 4 U - Turning 13 Entering or Leaving E E 10 Merging R ACTION: Ahead 5 Changing 11 Slowing or Stopping Driveway R (Check 2 Turning Right Lanes 12 Stopped in Traffic Lane 14 Pulling Out from Parking One) Space 3 Turning Left 6 Passing OWNER'S FULL NAME Same as ADDRESS CITY POINT OF IMPACT V O E Driver YEAR MAKE MODEL B LICENSE PLATE NUMBER STATE T H O H I DIRECTION OF D ROUTE 1 E C TRAVEL: N S E ON 2 (See LOCATION Section R L (If turning, enter (Or Street) E APPROXIMATE COST TO REPAIR AREA(S) SelectAbove) Number(s) from Diagram → $ Total Loss INITIAL ON O D DAMAGED PROPERTY OTHER THAN OF PAVEMENT Approx. Damage A VEHICLES PAVEMEN S E W T T FEET EDGE $ H M A OWNER'S NAME ADDRESS CITY STATE E G R E N Name Address Telephone Number W E I S T S
I Name and Address of Insurance Company -- Vehicle No. 2 (If uninsured, please indicate) N S INJURY CLASSIFICATION FIRST AID BY SEATING SEAT BELTS EJECTED 1 - None 1 - None Installed C K - Killed 1 2 3 M - Motorcycle 1 - No A - Bleeding Wound, Distorted 2 - Police B - Pedacycle 2 - Not Used 2 - Yes O Member, 3 - Emergency P - Pedestrian 3 - Lab Pelt Only Used 3 - Partially or Had to Be Carried from Medical 4 5 6 O - Other 4 - Lap and Shoulder Bellts 4 - Unknown D Technician Used Scene. 4 - Doctor NOTE: Positions 5 - Unknown E B - Bruises, Abrasions, Swelling, 5 - Rescue Squad 7 8 9 7, 8 1 - OCCUPANT OF YOUR VEHICLE S Limping, Etc. 6 - Helicopter and 9 indicate VEH. NO. C - No Visible Injury But Complaint Crew Rear 2 - OCCUPANT OF OTHER VEHICLE of 7 - Paramedic of Station Wagon. For each person injured or killed in the accident, use the codes above to fill in FIRS AGE SE VEH. IN- T SEAT SEAT EJEC the boxes at the right. X I NO. JURY AID ING BELTS TED N 1. Name Address
J DESCRIPTION OF INJURY: U 2. Name Address R I DESCRIPTION OF INJURY: E 3. Name Address S DESCRIPTION OF INJURY:
A 5 6 LEFT & RIGHT TURN SINGLE VEHICLE ACCIDENT C 1 Rear End C ACCIDENT OCCURRED ON OFF PAVEMENT 2 Head On I LEFT TURNS D 3 Same 7 8 9 10 11 12 E Direction N Sideswipe T 4 Opposite Direction RIGHT TURNS T Sideswipe Y 13 14 15 16 17 P E DESCRIBE WHAT HAPPENED (Refer to Vehicles by Numbers: State Vehicle = 1, Other Vehicle = 2) N A R R A T I V E
PEDESTRIAN ACTION: 1 Crossing at Intersection 4 Walking on Pavement Facing P 2 Crossing Not at Intersection Traffic 7 Working on Pavement E Clothing: Light 3 Walking on Pavement With 5 Standing on Pavement 8 Other on Pavement D Dark Traffic 6 Playing on Pavement 9 Not on Pavement
E LIGHT WEATHER ROADWAY ROAD TYPE TRAFFIC CONTROL VISION OBSCURED BY SURFACE N 1 Daylight 1 Clear 1 Blacktop 1 Stop Sign 1 Not Obscured 7 Hillcrest V 2 Dark 2 Cloudy 1 Dry 2 2 Traffic Signal 2 Rain, Snow, 8 Parked I 3 Dark, 3 Raining 2 Wet Concrete 3 Yield Sign R Ice Vehicle(s) Arti- 4 Fog, Smog 3 Snow, Ice 3 Brick 4 Officer, Flagman O 5 Snowing or on 9 Moving ficial 4 Muddy 4 Gravel 5 RR Gates, N Sleeting Windshield Vehicle(s) Lights 5 Hazardous 5 Dirt Signals M 4 Dusk 6 Hailing 3 Trees, Bushes 10 Blinding E Material 6 Other 6 None 5 Dawn 4 Building(s) Headlights N 5 Embankment T NUMBER 7 Other 11 Blinding Sunlight OF LANES: WERE LANES CLEARLY MARKED? YES NO Yes 6 Signboard 12 Other FUNCTIONING? No 13 Unknown DATE OF Operator THIS REPORT: SIGN HERE: Owner