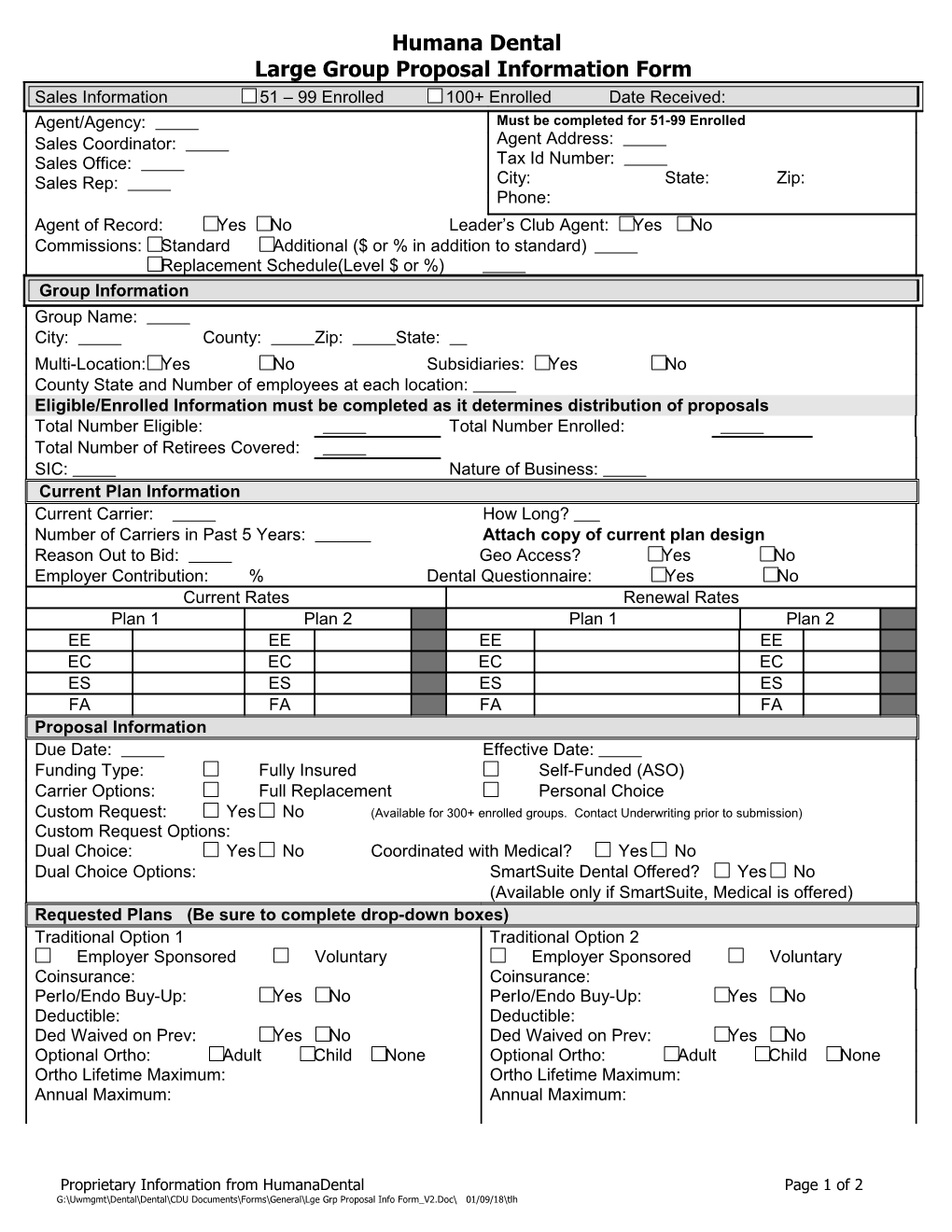
Humana Dental Large Group Proposal Information Form Sales Information 51 – 99 Enrolled 100+ Enrolled Date Received: Agent/Agency: Must be completed for 51-99 Enrolled Sales Coordinator: Agent Address: Sales Office: Tax Id Number: Sales Rep: City: State: Zip: Phone: Agent of Record: Yes No Leader’s Club Agent: Yes No Commissions: Standard Additional ($ or % in addition to standard) Replacement Schedule(Level $ or %) Group Information Group Name: City: County: Zip: State: Multi-Location: Yes No Subsidiaries: Yes No County State and Number of employees at each location: Eligible/Enrolled Information must be completed as it determines distribution of proposals Total Number Eligible: Total Number Enrolled: Total Number of Retirees Covered: SIC: Nature of Business: Current Plan Information Current Carrier: How Long? Number of Carriers in Past 5 Years: Attach copy of current plan design Reason Out to Bid: Geo Access? Yes No Employer Contribution: % Dental Questionnaire: Yes No Current Rates Renewal Rates Plan 1 Plan 2 Plan 1 Plan 2 EE EE EE EE EC EC EC EC ES ES ES ES FA FA FA FA Proposal Information Due Date: Effective Date: Funding Type: Fully Insured Self-Funded (ASO) Carrier Options: Full Replacement Personal Choice Custom Request: Yes No (Available for 300+ enrolled groups. Contact Underwriting prior to submission) Custom Request Options: Dual Choice: Yes No Coordinated with Medical? Yes No Dual Choice Options: SmartSuite Dental Offered? Yes No (Available only if SmartSuite, Medical is offered) Requested Plans (Be sure to complete drop-down boxes) Traditional Option 1 Traditional Option 2 Employer Sponsored Voluntary Employer Sponsored Voluntary Coinsurance: Coinsurance: PerIo/Endo Buy-Up: Yes No PerIo/Endo Buy-Up: Yes No Deductible: Deductible: Ded Waived on Prev: Yes No Ded Waived on Prev: Yes No Optional Ortho: Adult Child None Optional Ortho: Adult Child None Ortho Lifetime Maximum: Ortho Lifetime Maximum: Annual Maximum: Annual Maximum:
Proprietary Information from HumanaDental Page 1 of 2 G:\Uwmgmt\Dental\Dental\CDU Documents\Forms\General\Lge Grp Proposal Info Form_V2.Doc\ 01/09/18\tlh Humana Dental Large Group Proposal Information Form
Requested Plans (continued) PPO Option 1 PPO Option 2 Employer-Sponsored Voluntary Employer-Sponsored Voluntary Coinsurance: Coinsurance: Deductible: Deductible: Annual Maximum: Annual Maximum: Optional Ortho: Adult Child None Optional Ortho: Adult Child None Ortho Lifetime Maximum: Ortho Lifetime Maximum: Ded Waived on Preventive: Yes No Ded Waived on Preventive: Yes No Perio/Endo Buy-up Yes No Perio/Endo Buy-up Yes No Prepaid Option 1 Prepaid Option 2 Employer-Sponsored Employer-Sponsored Voluntary Voluntary Plan: Plan: Optional Ortho: Yes No Optional Ortho: Yes No Ortho Lifetime Maximum: $ Ortho Lifetime Maximum: $ Life/AD&D (Only complete if not quoting Medical STD: (Only complete if not quoting Medical and if and if Medical is not active with Humana) Medical is not active with Humana) Options: Benefits Schedule: Basic Level Weekly Amount $ Dependent Salary Schedule Voluntary Salary/Class Schedule
Benefit Schedule: Note: Minimum weekly amount = $100 Flat Amount $ Maximum weekly amount = $500 Salary/Class Schedule
Did you include: Dental census by coverage type and by group county location. Copy of the current dental benefit plan. (To include if Endo & Perio are in Basic? Deductible waived on Preventive?) Two complete years of dental enrollment and dental claims history, current to within 6 months of proposed effective date for 300+ groups Miscellaneous Comments:
Route all Dental hardcopy proposals to:
Humana, Inc. – Nicolet By Fax: (920)337-5281 Attn: Corporate Dental Underwriting 325 Reid Street DePere, WI 54115
Proprietary Information from HumanaDental Page 2 of 2 G:\Uwmgmt\Dental\Dental\CDU Documents\Forms\General\Lge Grp Proposal Info Form_V2.Doc\ 01/09/18\tlh