Adrenal Pathology
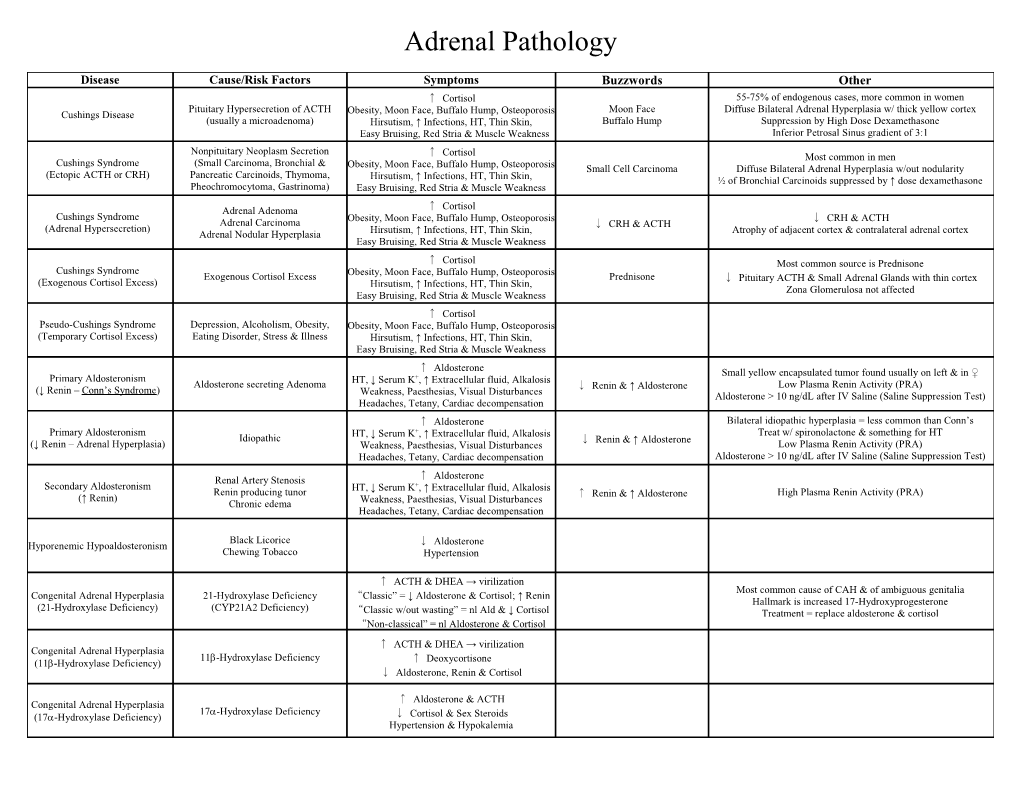
Disease Cause/Risk Factors Symptoms Buzzwords Other ↑ Cortisol 55-75% of endogenous cases, more common in women Pituitary Hypersecretion of ACTH Moon Face Diffuse Bilateral Adrenal Hyperplasia w/ thick yellow cortex Cushings Disease Obesity, Moon Face, Buffalo Hump, Osteoporosis (usually a microadenoma) Hirsutism, ↑ Infections, HT, Thin Skin, Buffalo Hump Suppression by High Dose Dexamethasone Easy Bruising, Red Stria & Muscle Weakness Inferior Petrosal Sinus gradient of 3:1 Nonpituitary Neoplasm Secretion ↑ Cortisol Most common in men Cushings Syndrome (Small Carcinoma, Bronchial & Obesity, Moon Face, Buffalo Hump, Osteoporosis Small Cell Carcinoma Diffuse Bilateral Adrenal Hyperplasia w/out nodularity (Ectopic ACTH or CRH) Pancreatic Carcinoids, Thymoma, Hirsutism, ↑ Infections, HT, Thin Skin, ½ of Bronchial Carcinoids suppressed by ↑ dose dexamethasone Pheochromocytoma, Gastrinoma) Easy Bruising, Red Stria & Muscle Weakness ↑ Adrenal Adenoma Cortisol Cushings Syndrome ↓ Adrenal Carcinoma Obesity, Moon Face, Buffalo Hump, Osteoporosis ↓ CRH & ACTH (Adrenal Hypersecretion) CRH & ACTH Adrenal Nodular Hyperplasia Hirsutism, ↑ Infections, HT, Thin Skin, Atrophy of adjacent cortex & contralateral adrenal cortex Easy Bruising, Red Stria & Muscle Weakness
↑ Cortisol Most common source is Prednisone Cushings Syndrome Obesity, Moon Face, Buffalo Hump, Osteoporosis Exogenous Cortisol Excess Prednisone ↓ Pituitary ACTH & Small Adrenal Glands with thin cortex (Exogenous Cortisol Excess) Hirsutism, ↑ Infections, HT, Thin Skin, Zona Glomerulosa not affected Easy Bruising, Red Stria & Muscle Weakness ↑ Cortisol Pseudo-Cushings Syndrome Depression, Alcoholism, Obesity, Obesity, Moon Face, Buffalo Hump, Osteoporosis (Temporary Cortisol Excess) Eating Disorder, Stress & Illness Hirsutism, ↑ Infections, HT, Thin Skin, Easy Bruising, Red Stria & Muscle Weakness ↑ Aldosterone Small yellow encapsulated tumor found usually on left & in ♀ Primary Aldosteronism + Aldosterone secreting Adenoma HT, ↓ Serum K , ↑ Extracellular fluid, Alkalosis ↓ Low Plasma Renin Activity (PRA) (↓ Renin – Conn’s Syndrome) Renin & ↑ Aldosterone Weakness, Paesthesias, Visual Disturbances Aldosterone > 10 ng/dL after IV Saline (Saline Suppression Test) Headaches, Tetany, Cardiac decompensation ↑ Aldosterone Bilateral idiopathic hyperplasia = less common than Conn’s Primary Aldosteronism HT, ↓ Serum K+, ↑ Extracellular fluid, Alkalosis Treat w/ spironolactone & something for HT Idiopathic ↓ Renin & ↑ Aldosterone (↓ Renin – Adrenal Hyperplasia) Weakness, Paesthesias, Visual Disturbances Low Plasma Renin Activity (PRA) Headaches, Tetany, Cardiac decompensation Aldosterone > 10 ng/dL after IV Saline (Saline Suppression Test) ↑ Renal Artery Stenosis Aldosterone Secondary Aldosteronism + Renin producing tunor HT, ↓ Serum K , ↑ Extracellular fluid, Alkalosis ↑ High Plasma Renin Activity (PRA) (↑ Renin) Renin & ↑ Aldosterone Chronic edema Weakness, Paesthesias, Visual Disturbances Headaches, Tetany, Cardiac decompensation
Black Licorice ↓ Hyporenemic Hypoaldosteronism Aldosterone Chewing Tobacco Hypertension
↑ ACTH & DHEA → virilization Most common cause of CAH & of ambiguous genitalia Congenital Adrenal Hyperplasia 21-Hydroxylase Deficiency “Classic” = ↓ Aldosterone & Cortisol; ↑ Renin Hallmark is increased 17-Hydroxyprogesterone (21-Hydroxylase Deficiency) (CYP21A2 Deficiency) “Classic w/out wasting” = nl Ald & ↓ Cortisol Treatment = replace aldosterone & cortisol “Non-classical” = nl Aldosterone & Cortisol ↑ ACTH & DHEA → virilization Congenital Adrenal Hyperplasia 11-Hydroxylase Deficiency ↑ (11-Hydroxylase Deficiency) Deoxycortisone ↓ Aldosterone, Renin & Cortisol
↑ Aldosterone & ACTH Congenital Adrenal Hyperplasia 17-Hydroxylase Deficiency (17-Hydroxylase Deficiency) ↓ Cortisol & Sex Steroids Hypertension & Hypokalemia Adrenal Pathology (contd.)
Disease Cause/Risk Factors Symptoms Buzzwords Other
Immediate steroid need 1) Immediate need for steroids – glands unable to respond Cortical Hypofunction Rapid steroid withdrawal ↑ 2) Rapid Withdrawal of steroids (Primary Acute Insufficiency) ACTH Mass Destruction (DIC,Hemorrhage) 3) Massive destruction – hemorrhage, anticoagulants, DIC
Waterhouse-Friderichsen Bacteremic Infection Adrenal Hemorrhage → Cortical Hypofunction ↑ More common in children Syndrome ACTH
Autoimmune (majority) Destruction of adrenal cortex only Cortical Hypofunction TB, Histoplasmosis, Carcinoma Fatigue, muscle weakness, weight loss, GI upset (Primary Chronic Insufficiency) ↑ Thin cortex w/ lymph infiltrates – unaffected medulla AIDS, Amyloidosis, Sarcoidosis Hypoglycemia, Salt craving, Prerenal Azotemia ACTH (Addison’s Disease) Hemochromatosis Acidosis, Hypotension & Hyperpigmentation Cortical Hypofunction Autoimmune (majority) (Primary Chronic Insufficiency) TB, Histoplasmosis, Carcinoma 1) Adrenal insufficiency – same as above ↑ Thin cortex w/ lymph infiltrates – unaffected medulla (Addison’s Disease) AIDS, Amyloidosis, Sarcoidosis 2) Hypoparathyroidism & Candidiasis ACTH Subtype I Hemochromatosis Cortical Hypofunction Autoimmune (majority) (Primary Chronic Insufficiency) TB, Histoplasmosis, Carcinoma 1) Adrenal insufficiency – same as above ↑ Thin cortex w/ lymph infiltrates – unaffected medulla (Addison’s Disease) AIDS, Amyloidosis, Sarcoidosis 2) Autoimmune thyroid disease & Type I DM ACTH Subtype II– Schmidt’s Syndrome Hemochromatosis
Cortical Hypofunction Congenital Adrenal Hyperplasia (Primary Chronic Insufficiency) ↑ Enzyme Inhibitor (ex. = ketoconazole) ACTH (Failure of Cortisol Production)
Carcinoma, Infection, Irradiation, No aldosterone or ACTH deficiency Cortical Hypofunction Fatigue, muscle weakness, weight loss, GI upset Infarction Features of panhypopituitarism (Chronic 2º/3º Insufficiency) Hypoglycemia, Salt craving, Prolonged use of steroids→↓ ACTH Delayed response to prolonged ACTH stimulation test
HT with or without paroxysmal attacks Most are solitary & in medulla; pink colored; large = encapsulated Headaches, sweating, fever, GI upset, anxiety Diagnosis = Normetanephrine & metanephrine in plasma Pheochromocytoma MEN Type II or III Adrenomedullary Chromafin cells Palpitations orthostatic HT, numbness Clonidine useful in exclusion; Paroxysms can be provoked Cardiac manifestations Rule of 10’s = 10% extrarenal, bilateral, malignant, familial
Parathyroid hyperplasia MEN Syndrome Type I Pituitary adenomas (Wermer Syndrome) Pancreatic islet tumors
Pheochromocytoma MEN Syndrome Type II MEN IIA = Parathyroid Adenoma Medullary Thyroid carcinoma (Sipple Syndrome) MEN IIB = Mucocutaneous ganglioneuromas & Marfanoid habitus Parathyroid hyperplasia
Pheochromocytoma MEN Syndrome Type III Medullary Thyroid carcinoma Mucosal neuromas/Marfanoid features Endocrine Pancreas Pathology Disease Cause/Risk Factors Symptoms Buzzwords Other Blindness (Lens, Retina, Optic Nerve) Genetic (HLA-DR3 &4) MI is #1 cause of death; Diabetic ketoacidosis Primary Diabetes Mellitus CV disease (MI, stroke, gangrene) HLA-DR3&4 Autoimmune Antibodies Glycosylated collagens →Advanced Glycosylation End Products Type I Nephropathy & Infections (Mucomycosis) Diabetic ketoacidosis Environment (Viral Infection) Intracellular hyperglycemia→Sorbitol (lens & Schwann Cell) Peripheral Neuropathy, Polydipsia & Polyuria Genetic (not HLA related) Blindness (Lens, Retina, Optic Nerve) MI is #1 cause of death; Hyperosmolar Coma Primary Diabetes Mellitus Obesity CV disease (MI, stroke, gangrene) Hyperosmolar Coma Glycosylated collagens →Advanced Glycosylation End Products Type II Insulin Deficiency Nephropathy & Infections (Mucomycosis) Intracellular hyperglycemia→Sorbitol (lens & Schwann Cell) Insulin Resistance (receptor & GLUT) Peripheral Neuropathy, Polydipsia & Polyuria
Pancreatitis Secondary Diabetes Mellitus Pancreatic Cancer Destruction of islets after disease Drugs
Thyroid Pathology Disease Cause/Risk Factors Symptoms Buzzwords Other Dietary Hyperplastic enlargement of thyroid Diffuse Non-Toxic Goiter ↓ Involves whole gland iodine ↓ T3/T4 (Endemic) goitrogens More common ↑ TSH
Hyperplastic enlargement of thyroid Diffuse Non-Toxic Goiter Substance interfering with synthesis ↓ T3/T4 Young females Typically young females (Sporadic) Hereditary enzyme defect ↑ TSH
Hyperplastic enlargement of thyroid ↓ Nodules/Cysts Multinodal Goiter T3/T4 & ↑ TSH Hemorrhage, scarring & calcification Recurrent hyperplasia & involution Irregular Irregular with Nodules & Cysts
Toxic multinodal goiter Plummer’s Syndrome Hyperfunctioning Goiter ↑ T3/T4 No skin/eye changes of Grave’s Disease
Thyrotoxicosis (with diffuse hyperplasia) Typically females Autoimmune (LATS/TSI & TGI) Graves Disease Ophthalmopathy (Paralysis & exopthalmos) Treatment: PTU, methimazole, radioiodine & surgery Genetic? (HLA-B8 & DR3) Dermopathy (Pretibial myxedema) Eye Muscle Paralysis & Exopthalmos NOT seen in Thyrotoxicosis
Cardiac: ↑HR,A-fib,Cardiomegaly, CHF Low TSH (suggestive) & High T4 (confirms) Hyperfunctioning Thyroid Heat Intolerance Neuromuscular: Hyperreflexia,tremor,wasting Hyperpigmentation over extensor surfaces Thyrotoxicosis Leakage from Thyroid Lid Lag Skin: Heat Intolerance, ↑ Sweat & Pigmentation Uncommon causes: Hydatiform mole, Struma ovarii, carcinomas Ingestion of iodide or Synthroid ↓ Cholesterol ↑ Appetite, GI motility, Osteoporosis, Eyes Treatment: Blockers, Propylthiuracil (PTU) , Iodide, Ablation Insufficient Parenchyma Anemia, ↑ Cholesterol, ↓ Na , Myxedema + High TSH (suggestive) & Low Free T4 (confirms) Hashimoto Thyroiditis (Autoimmune) Cold Intolerance, Fatigue, Depression, Lethargy ↑ Primary Hypothyroidism Cholesterol Therapy = T4 replacement (TSH takes 6-8 weeks to normalize) Developmental, Radiation Weight ↑, Edema, Constipation, Cardiomyopathy Myxedema Low TSH after Tx → osteoporosis & arrythmias Ablation Delayed reflexes (achilles) & Coma (If severe)
TSH is unreliable; Use T4 to make diagnosis Seondary Hypothyroidism Pituitary Lesion TRH stimulation Test = no response
TSH is unreliable; Use T4 to make diagnosis Tertiary Hypothyroidism Hypothalamic Lesion TRH stimulation Test = delayed response (60 min)
↓ Synthesis Hypothyroidism - Other Idiopathic (block of TSH receptors Use increased dose of T4 during pregnancy Heriditary, Hashimoto Thyroiditis Lithium, Iodides, p-aminosalicylate Mental Retardation Infant Hypothyroidism Short Stature, Coarse Facial Features Protruding Tongue Cretinism Early Childhood Hypothyroidism Umbilical Hernia Umbilical Hernia Protruding Tongue Delayed Brain Development Thyroid Agenesis Deafness & Mutism Fetal Hypothyroidism Iodine Deficiency Deaf & Mute Spasticity Congenital Synthetic Defect Severe Mental Retardation Thyroid Pathology (contd) Disease Cause/Risk Factors Symptoms Buzzwords Other TPO Antibodies (99% sensitive) Female Predominance Diffusely but painlessly enlarged Thyroid Chronic Autoimmune Thyroiditis Deficiency of Suppressor T Cells Early transient Thyrotoxicosis Early transient Thyrotoxicosis, Later Hypothyroidism Lymph infiltrates & follicles (Hashimoto Thyroiditis) Genetic? (HLA-DR3 &5) Later Hypothyroidism Risk for B Cell Lymphomas Hurthle Cells (granular cytoplasm) TSH antibodies blocking receptor Other antibodies: Thyroglobulin, Thyroid Peroxidase, I transporter
Subacute Thyroiditis Painful, diffusely enlarged Thyroid Viral (Mumps, Influenza, Coxsackie) Painful Self Limited (DeQuervain’s/Granulomatous) Giant Cells & Macrophages (like granuloma)
Vigorous Palpation Palpation Thyroiditis Giant Cells & Macrophages (like granuloma) Disuption of follicles
Subacute Lymphocyte Self Limited Idiopathic Painless Goitrous Enlargement Post-Partum Thyroiditis Often seen in post-partum women
Causes Laryngeal Nerve Paralysis (SOB & difficulty swallowing) Fibrosing Thyroiditis - Painless Riedel’s Thyroiditis Simulates malignancy Hard gland May be associated with fibrosis elsewhere
Majority of Thyroid neoplasms Benign, solitary, encapsulated Follicular Adenoma Not likely to cause thyrotoxicosis Doesn’t take up iodine May make more T3 than T4
Encapsulated or Infiltrating Most common thyroid cancer –↑ incidence in Gardner Syndrome RET gene mutation (MEN II) Radiation Complex branching papillae Optically clear nuclei in “Little Orphan Annie Cells” Papillary Carcinoma RAS gene mutation Little Orphan Annie Optically Clear nuclei & Psammoma bodies Metastisize to regional nodes; Usually indolent growth Radiation exposure (most common) Nodal Metastasis Intranuclear inclusions, grooves Treatment = Thyroidectomy & radioiodine therapy, Survival 98%
2nd most common - Survival 92% Invasion Follicular Carcinoma RAS gene mutation Vascular or Capsular Invasion Hematogenously spread to bone, lungs & brain Blood Metastasis Treatment lobectomy or thyroidectomy, radioiodine (if invasive)
Hurthle Cell Neoplasm RAS gene mutation Abundent granular cytoplasm Behave the same as follicular cell carcinoma/adenoma (Adenoma or Carcinoma)
Parafollicular C Cells (neuroendocrine) Rare – most sporadic, 20% as MEN II or familial Amyloid Stroma RET gene mutation (MEN II) Nodule or multifocal May be paraneoplastic (CEA, somatostatin, serotonin & VIP) Medullary Carcinoma Calcitonin RAS gene mutation Not encapsulated, round or spindle cells Metastasize in blood to lung, liver, bone & nodes Not encapsulated Amyloid( Calcitonin) tumor stroma Treatment = Thyroidectomy Poor prognosis – uniformly fatal RAS gene mutation Undifferentiated neoplasms Elderly Loss of I uptake & ↓ Thyroglobulin Anaplastic Carcinomas P53 gene mutation Large, locally invasive, rapidly growing Fatal Survival less than 1 year from diagnosis Possibly derived from Papillary Carcinoma Leukemia & Lymphoma Disease Cause/Risk Factors Symptoms Buzzwords Other Trisomy 21, Bloom’s, Fanconi’s Rapid Onset, > 20% Blasts Cells similar to lymphoblastic lymphoma Children Acute Lymphoblastic Leukemia Radiation Bone Pain, CNS & Testes Involvement Generally good prognosis (70%) = ↓ WBC, t12:21, < 9yo, diploidy TdT+, (ALL) Alkylating Agents, Benzene HSmegaly, Anemia & Thrombocytopenia Bad = WBC (>10K), T-Type, t9:22, 11q23, organomegaly Scant agranular cytoplasm Viral T Type = lymphadenopathy & mediastinal mass 3 types: Pre B (85%), Pre T (15%), B “like Burkitts” (2%) Trisomy 21, Bloom’s, Fanconi’s Rapid Onset, > 20% Blasts Fair prognosis (40%), Usually adults Auer rods Acute Myeloid Leukemia Radiation Anemia & Thrombocytopenia Frequent infections & mucosal bleeding CD13, CD15, CD33 (AML) Alkylating Agents, Benzene Monocytic = gum hyperplasia Good = t8:21, t15:17 (treat w/ RA) & Chrom 16 abnormalities Granular Cytoplasm Viral Promyelocytic (M3) = DIC, ↓WBC Bad = t9:22, 11q23, origin from myelodysplasia or treatment Trisomy 21, Bloom’s, Fanconi’s Acute Leukemia Radiation Myeloid & Lymphoid features Poor prognosis of Ambiguous Lineage Alkylating Agents, Benzene Viral Trisomy 21, Bloom’s, Fanconi’s Gradual onset, Mature Cells Usually adults, Philadelphia Chromosome (t 9:22) ↓ Chronic Myeloid Leukemia Radiation 100% cellular Bone Marrow (no fat) LAP bcr-abl ↑ Tyrosine Kinase activity ( Treat with Gleevec) t9:22 or bcr-abl (CML) Alkylating Agents, Benzene Pluripotent Stem Cells→Granulocytes ↓ Leukocyte Alkaline Phosphatase (LAP) Pluripotent Stem Cells Viral Splenomegaly = Draggin Sensation Poor Prognosis - Always goes to blast crisis (AML or ALL) Gradual onset, Mature Cells, Hepatosplenomegaly Not radiation Usually adults (most common adult leukemia in west) Trisomy 21, Bloom’s, Fanconi’s Chronic Lymphocytic Leukemia Clonal B Cell Disorder (small lymphocytes) CD5, CD20, CD23 Same as CLL; indolent, not affected by therapy Alkylating Agents, Benzene (CLL) ↑ Del 13q Some have large cell transformation (Richter Syndrome) Viral Infections Hypogammoglobulinemia RichterSyndrome Bad = trisomy 12, CD38 & de1 11q Gradual onset Adult Men Usually adult men (2% of leukemias) Trisomy 21, Bloom’s, Fanconi’s Hairy Cell Leukemia Bacterial & Mycobacterial Infections Not radiation Fair prognosis (40%) Alkylating Agents, Benzene (HCL) Beefy Red Splenomegaly, ↑ Reticulin in BM “ Pancytopenia (70%), Neutropenia & Monocytopenia (90-100%) Viral Fried Egg appearance” TRAP+ B Cells TRAP+ Good Treatment - 2-CDA, pentostatin & interferon Many subtypes based on ringed sideroblasts & blast counts BM = Hypercellular, Periphery = Pancytopenia Idiopathic Ringed Sideroblasts May progress to AML Myelodysplastic Syndrome <20% blasts in BM, Megaloblastic appearance Therapy related (ex. Radiation) Chromosome 5,7,8 Very poor prognosis Anemia, Infection, Hemorrhage Chromosome 5,7,8 abnormalities ↓ erythropoietin Early organomegaly due to congestion ↑ RBC, Platelets & Granulocytes ↑ Hematocrit Late organomegaly due to extramedullary erythropoiesis Polycythemia Vera Growth Factor Mutations Fibrotic Marrow, Hypertension, Pruritis, Gout Hypertension & Hemorrhage Spent Phase = Fibrotic Marrow DVT, MI, Stroke ↑ Viscosity Fair to good prognosis (depends on treatment-phlebotomy) Early progression to myelofibrosis (spent phase) Dacrocytes (teardrop cells) & enlarged platelets in periphery PDGF & TGF- Chronic Idiopathic Myelofibrosis Pancytopenia & Etramedullar hematopoiesis “ Dacrocytes Sensation of fullness” (Agnogenic Myeloid Metaplasia) Excess collagen from fibroblasts Reticulin Prognosis is difficult to predict Markedly enlarged spleen, Gout Transformation ot AML (20%)
Marked Thrombocytosis (>600,000) Least common of myeloproliferative disorders Large Platelets Essential Thrombocythemia Idiopathic Large Platelets Diagnosis by exclusion No myelofibrosis Thrombosis & Hemorrhage Good prognosis (>10 year survival)
No Typical Reed Sternberg Cells Predominance of lymphocytes/hystiocytes Men more common Hodgkin’s Disease Lymphohystocytic Cells EBV Typically a cervical node Best Prognosis (Lymphocyte Predominance) B Cell Lymphoma Cd20 & CD45 Can turn into Diffuse Large B Cell Lymphoma CD20 & CD45
Hodgkin’s Disease Predominance of lymphocytes/hystiocytes No Typical Reed Sternberg Cells Men more common EBV (Lymphocyte Rich) CD15 & CD30 Lymphohystocytic Cells Can turn into Diffuse Large B Cell Lymphoma Leukemia & Lymphoma (Contd.) Disease Cause/Risk Factors Symptoms Buzzwords Other
Cervical, Supraclavicular or mediastinal nodes Lacunar Reed Sternberg Cells Hodgkin’s Disease Most common type; affects adolescent or young adult women EBV Variable cell composition & necrosis Collagen Bands (Nodular Sclerosis) Staging (usually I or II) determines treatment; Good prognosis CD15 & CD30 Women
Variable cell composition & focal necrosis Hodgkin’s Disease Disordered fibrosis 2nd most common type; men more common EBV Classic Reed Sternberg Cells (Mixed Cellularity) Eosinophils, Plasma & T Cells Staging determines treatment; Guarded prognosis CD15 & CD30 1) Diffuse Fibrosis – RS Cells embedded in Fairly common – usually in older patients Poor Prognosis Hodgkin’s Disease fibrous stroma Often Bone Marrow Involvement (Stage III or IV) EBV Many Reed Sternberg Cells (Lymphocyte Depletion) 2) Reticular – RS Cells in sheets Poor prognosis Bone Marrow ↑ #s of Reed Sternberg Cells Usually not a true Hodgkin’s Lymphoma? Gradual onset, Mature Cells, Hepatosplenomegaly Not radiation Usually adults (most common adult leukemia in west) Trisomy 21, Bloom’s, Fanconi’s Clonal B Cell Disorder (small lymphocytes) CD5, CD20, CD23 Same as CLL; indolent, not affected by therapy Small Lymphocytic Lymphoma Alkylating Agents, Benzene ↑ Del 13q Some have large cell transformation (Richter Syndrome) Viral Infections Hypogammoglobulinemia RichterSyndrome Bad = trisomy 12, CD38 & de1 11q Nodular Growth Pattern with 2 cell types 1) Centrocytes = cleaved nuclear contours CD10,CD20,CD23 Fairly Common; indolent, not affected by therapy Follicular Lymphoma 2) Centroblasts = clear chromatin & multinucleate BCL-2, t14:18 May transform to diffuse large B cell lymphoma Bone Marrow frequently involved
Atrophied germinal center CD5 & CD20 Mantle Cell Lymphoma Not indolent or treatable Small cells with cleaved nuclear contour BCL-1, t11:14
Marginal Zone B-Cell Lymphoma H. Pylori Large B Cells, some plasma cells CD20 Common in GI Tract, Indolent, not dependent on treatment (MALT Type) Autoimmune (Sjogren, Hashimoto)
Very Common, Very Aggressive EBV T14:18, t8:14, t13:14 Prognosis depends on treatment, BCL-6 = good prognosis Diffuse Large B-Cell Lymphoma Large cell size, diffuse growth pattern HSV8 BCL2,C-Myc,BCL6
One of three bad types in kids “ Starry Sky picture” Highest growth fraction of all tumors Burkitt’s Lymphoma EBV “ Starry Sky picture” CD10,CD19,CD20 Most manifest as extra-nodal sites C-Myc Responsive to treatment, but poor prognosis
Lymphoblastic Lymphoma One of three bad types in kids Mediastinal Mass like Hodgkins CD3, TdT+, TCL-1 (T Type) (T/B) Responsive to treatment, but poor prognosis
One of three bad types in kids Anaplastic Large T/Null Cell CD3, CD30 Uncommon in adults, Common in children Lymphoma ALK, EMA t2:5 Presents in extra-nodal tissue Usually T, not B cell
Extranodal NK/T Cell Lymphoma Peripheral T-Cell Lymphoma EBV CD3 Poor Prognosis; Common in Asia, uncommon in US Nasal Type – eats face off Leukemia & Lymphoma (Contd. 2) Disease Cause/Risk Factors Symptoms Buzzwords Other
Indolent Cutaneous disorder CD4 Mycosis fungoides Cerebriform nuclei Extracutaneous spread Polyclonal Ig (Leukemia = Sezary Syndrome)
Painful Bone Destruction, ↓ Humoral Immunity M Protein Radiation, Chemicals, Asbestos Most common 1º malignant tumor of bone Plasmacytosis with IL-6, Vertebral Fractures Bence Jones Protein Multiple Myeloma Black Race Complications: Renal failure, Amyloidosis, AML (rarely) M Protein, Bence Jones proteins, Hypercalcemia Hypercalcemia HSV8? Fair prognosis (3 yr) Can spread to nodes, skin, etc IL-6 Plasmocytosis with ↑ Light Chain Production Radiation, Chemicals, Asbestos Fibrils of -pleated sheets that stain Congo Red 1º Amyloidosis Black Race Large Tongue Usually immunoglobulin light chain Large tongue, Neuropathy, GI Multiple Myeloma Arrythmias, CHF
Fibrils of -pleated sheets that stain Congo Red HSmegaly, 2º Amyloidosis Chronic Infection or Inflammation HSmegaly, Proteinuria Proteinuria
Most common monoclonal gammopathy Monoclonal Gammopathy of Diagnosis of exclusion, IgG < 3.5 Aging M Proteins without other symptoms Undetermined Significance May develop into multiple Myeloma Requires no treatment
Pituitary Pathology Disease Cause/Risk Factors Symptoms Buzzwords Other
↑ Prolactin Most common secretory adenoma of anterior lobe Prolactinoma Amenorrhea, Galactorrhea, Infertility, Effects less obvious in postmenopausal women Loss of Libido Treated with bromocriptine
Injury to pituitary stalk Compression ↑ Due to decreased dopamine to the anterior lobe Hyperprolactinemia Prolactin Prolactin Trauma to Hypothalamus, Infection Non-prolactin secreting adenomas may compress stalk Drugs (Phenylthiazines) ↑ Growth Hormone → ↑ Hepatic IGF-1 Second most common secretory adenoma of anterior lobe Somatotroph Adenoma Some produce prolactin as well IGF-1 Treatment = transsphenoidal resection, bromocriptine & radiation Acromegaly (adults) & Gigantism (children) Acromegaly = hands, feet, face skin & viscera DM, HT, CHF, arthritis, weakness, GI carcinoma
↑ ACTH→ ↑ Cortisol (Cushing’s Disease) ACTH 90% are microadenomas Corticotroph Adenoma Moon facies, central obesity, striae, bruising Microadenoma Treatment = transsphenoidal resection Osteoporosis, DM & HT
Gonadotroph Adenoma No clinical syndrome Secrete hormones inefficiently and variably
Thyrotroph Adenoma Rarest
Pregnancy & Lactotroph Hypertrophy Sheehan’s Syndrome Hypotension, DIC Hypopituitarism Most common cause of anterior lobe ischemic necrosis Sickle Cell Anemia, ↑ ICP
Maldevelopment of diaphragma sella Depends on number of residual cells Pituitary Apoplexy Empty Sella Syndrome Hypopituitarism Maldevelopment = Arachnoid Herniation via enlarged opening Sheehan’s Syndrome No syndrome Ablation Interruption of DA to Posterior Lobe Trauma Diabetes Insipidus Large volume of dilute urine ↓ Treatment = Administer ADH Tumor ADH Inflammation Ectopic ADH (Small Cell Carcinoma) Syndrome of Inappropriate ADH Lung Disease (TB) Water Retention, Hyponatremia Treatment = Water Restriction, Slow normalization of Na+ ↑ (SIADH) Intracranial Lesions (↓ Inhibition) GI Upset, Cerebral Edema ADH (Rapid Normalization can cause Central Pontine Myelinolysis) Drugs
Hyperpituitarism, Hypopituitarism Hypothalamic Tumors Glioma & Craniopharyngioma are most common Diabetes Insipidus CNS Pathology Disease Cause/Risk Factors Symptoms Buzzwords Other
Reversible Concussion Blunt non-penetrating injury Paralysis Reversible Traumatic Paralysis Ocurring Immediately After Injury Immediate
Seizures Most common sites: Frontal Pole, Temporal Pole, Medial orbital Stress on parenchymal vessels Cognitive & Personality Changes surface of the temporal lobe Contusion Coup Intact pia-glial membrane Headaches Pia-arachnoid not penetrated Countercoup Dizziness Occur at crests of gyri
Subarachnoid bleeding Traumatic disruption of pia-arachnoid and brain surface Lacerations Penetrating Wounds Satellite petichial hemorrhages Meningocerebral cicatrix Meningocerebral cicatrix (glial scar) = epileptogenic focus Edema in tissue
Fracture Immediate Loss of Consciousness Collection of blood between dura and skull Epidural Hemorrhage Most = Arterial (Middle Meningeal) Lucid Interval Lenticular shaped hematoma Rarely = Dural Sinus, Bridging Veins Later Loss of Consciousness
Superficial Cortical Bridging Veins 48 hours-days; appears as clotted blood More Common than epidural hemorrhage Dural Sinus Laceration Gradual Loss of Consiousness Acute Subdural Hemorrhage Clotted Blood Typically seen in infants, elderly & alcoholics Depressed Fractures Hemiparesis → Hemiplegia Sheet of blood between dura & arachnoid; forms hyaline sac Bullet Wounds Evidence of Herniation (if > 60 cc) Superficial Cortical Bridging Veins Clotted & Fluid Blood More Common than epidural hemorrhage Dural Sinus Laceration Gradual Loss of Consiousness Subacute Subdural Hemorrhage Clotted & Fluid Blood Typically seen in infants, elderly & alcoholics Depressed Fractures Hemiparesis → Hemiplegia Sheet of blood between dura & arachnoid; forms hyaline sac Bullet Wounds Evidence of Herniation (if > 60 cc) Superficial Cortical Bridging Veins > 3 weeks & Liquefied Hematoma More Common than epidural hemorrhage Dural Sinus Laceration Gradual Loss of Consiousness Liquefied Hematoma Typically seen in infants, elderly & alcoholics Chronic Subdural Hemorrhage Depressed Fractures Hemiparesis → Hemiplegia Minor Precipitating Event Sheet of blood between dura & arachnoid; forms hyaline sac Bullet Wounds Evidence of Herniation (if > 60 cc) Slow Bleeding, No immediate symptoms, Minor precipitating event Trauma Superficial Cortical Veins Stiff Neck, Alterations in Consciousness Subarachnoid Hemorrhage Stiff Neck Usually multiple and small Surface cortical lacerations Vasospasm & Hydrocephalus Surface cortical contusions
Not in contact with the cortical surface, usually solitary Intracerebral Hematoma Rupture of Intrinsic Cerebral Vessels Frontal & Temporal Lobes are most common sites
Damage usually occurs where nerves exit through foramina Cranial Nerve Damage Cranial Fractures Most Common = CNI, CNII, CN V & CN VI
Pontomedullary Avulsion Marked Hyperextension of neck Poor prognosis, Immediately fatal if complete, die later if incomplete
Unconscious from moment of impact Diffuse Axonal Injury No lucid interval Results in disconnection of distal axonal segment Diffuse Shearing of axons Calpain (1º Axotomy) Ca2+ influx & swelling Most common sites = Corpus Callosum & S. Cerebellar Peduncles Microtubule depolymerization, Calpain activation CNS Pathology (Contd.) Disease Cause/Risk Factors Symptoms Buzzwords Other Unconscious from moment of impact Diffuse Axonal Injury No lucid interval Results in disconnection of distal axonal segment Small axonal membrane tears that reseal Axoplasmic Transport (2º Axotomy) Ca2+ activated proteases, repair fails Most common sites = Corpus Callosum & S. Cerebellar Peduncles Axoplasmic transport causes swelling
Greatest Damage = Hippocampus, Caudate, Putamen, Hypoxic Brain Injury Cortical Layers 3 & 5, Purkinje Cells of Cerebellum Diffuse or localized to watershed zone
Mechanical Damage White Matter Swelling White matter swelling adjacent to contusion Brain Swelling Blood Vessel Impairment Diffuse Swelling Diffuse Swelling of One or Both Hemispheres Vasodilation
Frontal & Temporal Lobes (White Matter) Multiple Petechial Hemorrhages Acceleration/Deceleration? Thalamus Usually seen in patients who die soon after head injury Brainstem
3-4 d = white matter petichiae, capillary necrosis Fractures of Limbs or Limb Giurdles 4-7d = grey matter alterations, fat in capillaries Fat Embolism Usually only seen in adults (children have less fat) (Fat enters veins) 12d-3m = many infarcts in cortex & pons >3 m = atrophy of white matter
Occurs during first week Early Post Traumatic Epilepsy Within first week More common in children than adults Associated with: Hematoma, Depressed Fracture, Amnesia
Most common complication of blunt head injury Occurs later than one week Late Post Traumatic Epilepsy Blunt Head Injury After first week ↑ Risk = Hematoma, Depressed Fracture, Early Epilepsy
T-Cell Autoimmune against Myelin Diagnosis = 2 lesions & 2 symptoms Young Women, CNS Commonest in young women; Affects CNS myelin, Variable course Unknown Visual Impairment, Weakness, Dysarthria Plaques Acute Plaque: Sharp Border, Inflammation & Edema, Demyelination Multiple Sclerosis Distance from equator, Environment Ataxia, Vertigo, Urinary Symptoms Variability Inactive Plaque: Sharp Border, No Inflammation Edema or Myelin Genetic CSF = ↑ Mono’s & IgG (OCB-not in serum) Oligoclonal Bands (OCB) Shadow Plaque: Poor Border, Thin Myelin at Periphery
Devic Disease Severe necrotic lesions in spinal cord and optic nerve only Spinal Cord & CN II Only (Neuromyelitis Optica) Rapidly progressive
Acute Multiple Sclerosis Fatal in 1-6 months (Marburg Type) Severe & Rapid with extensive involvement of brain & spinal cord
Rapid Correction of Hyponatremia Symmetric demyelination in the center of the base of the pons Sever Electrolyte Imbalance Central Pontine Myelinolysis Rapidly evolving quadriplegia CNS Can affect tegmentum occasionally Alcoholism, Liver Transplant Outcome is variable: Complete Recovery→Fatal Burns, Malnutrition Acute Influenza-like Illness Inflammation/Demyelination of Nerves & roots Treatment: Supportive, Plasmapheresis, IV Immunoglobulin CMV & Campylobacter jejuni PNS Guillian-Barre Syndrome Cranial & Spinal Motor Roots = Severe Outcome: Complete recovery is most common, rarely fatal Immunization Ascending Paralysis Ascending Paralysis Death due to respiratory paralysis Autoimmune? CNS Pathology (Contd. 2) Disease Cause/Risk Factors Symptoms Buzzwords Other Usually assymptomatic Non-closed vertebral arches without cyst Spina Bifida Occulta Folate Deficiency Stigmata (Hypertrichosis) Variable cord anomaly Stigmata: Hypertrichosis,Dimple,Lipoma,Nevus Sacral, Anorectal or UG Defect Meningocele: Meninges protrude through vertebral defect Non-closed vertebral arches with cyst Myelomeningocele: Meninges & Spinal cord protrude through defect Spina Bifida Cystica Folate Deficiency Cyst Meningocele or Myelomeningocele Most survive > 1 year, but frequently have progressive deterioration Disabilities are usual: paraplegia, incontinence, infection, learning 1) Myelomeningocele 2) Elongation of Inferior Vermis & Brain Stem with displacement i Arnold-Chiari Type II Mental Retardation into spinal canal 3) Hydrocephalus
Most common congenital malformation of the brain Annencephaly Folate Deficiency Absence of cerebrum & calvarium Stillborn or die shortly after birth
Most common neonatal intracranial hemorrhage Intraventricular Hemorrhage Preterm Birth Preterm PV Germinal Matrix is fragile, fibrinolytic & persists until 34 weeks (IVH) Periventricular Germinal Matrix Periventricular Germinal Matrix Variable: May be focal & asymptomatic, may spread into ventricles
Common ischemic lesion of preterm infant Initially non-specific Periventricular Leukomalacia Infarction of Periventricular White Matter Preterm Centrum Ovale = vulnerable boundry zone Later: Spastic Motor Dysfunction (PVL) (Centrum Semiovale) Centrum Semiovale (Ventriculopetal & Ventriculofugal Arteries) Paraplegia/Quadraplegia develops in surviving Usually not without permanent sequelae
Diffusely Infiltrative 20% of gliomas, Rarely Resectable, Progress towards anaplastic Diffusely infiltrate w/o clear margins Diffuse Astrocytoma No Clear Margins Graded on: Hypercellularity, endothelial changes & necrosis Found in white matter of cerebrum Cerebrum Poor Prognosis
Occur in Pons, infiltrate widely Brainstem Glioma Children (2nd decade) Range of grades includes glioblastoma CN Palsies, Long Tract signs, Gait abnormalities (Atrocytoma Subgroup) Pons Surgical removal not possible Emesis & Cerebellar Signs
Circumscribed Circumscribed, low grade, histology = biphasic Midline Young>Old Pilocytic Astrocytom Cerebellum, Hypothalamus, Optic Chiasm/Nerve Rosenthal Fibers Optic Nerve Gliomas associated with Von Recklinghausen’s (NF I) Rosenthal Fibers Von Recklinghausen’s (NF I)
60% cystic Most common astrocytoma of childhood Cerebellar Pilocytic Astrocytoma Children (2nd decade) Endothelial proliferation & pleomorphism Good Prognosis
Intraventricular Vascular Intraventricular Mass Subependymal Giant Cell Tumor Tuberous Sclerosis Benign but cause problems due to location & hemorrhaging Cells = Large, mix between astrocyte & neuron Hemorrhage
Supratentorial Common Most common glioma, Usually in older adults Rapid growth, endothelial proliferation, necrosis Adults Most invasive & aggressive, highly infiltrative Glioblastoma Multiforme Hemorrhagic Foci, Often zones of mixed tumor Always Recurs Tumor always recurs with resection, poor prognosis May Metastasize (CSF) Metastasis Mix: Oligodendroglioma,Ependymoma,Astrocytoma,Neuroectederm CNS Pathology (Contd. 3) Disease Cause/Risk Factors Symptoms Buzzwords Other
Focal Calcification Unusual in children Cerebral White Matter, Focal Calcification Oligodendroglioma LOH 1p, LOH 19q Good = both LOH 1p & 19q Fried Egg Appearance, Highly vascularized CDKN2A Bad = CDKN2A
Ventricular System (4th Ventricle is usual) 4th Ventricle All ages, but more often young>old & children = infratentorial Rosette & Pseudorosette Arrangement NF II Ependymoma Most common spinal intramedullary glioma, Associated w/ NF II Vascularized, differentiated & demarcated Rosettes & Pseudorosettes Best to Worst: Spinal Cord, Cerebrum, Posterior Fossa May Metastasize Metastasis Cauda Equina Fila Terminale Rare in Children, Usually benign Myxopapillary Ependymoma Mucinous Degeneration of Stroma Adults Can be locally destructive, Metastatic & can recur Mucinous Degeneration of Stroma
Usually 4th Ventricle Subependymoma 4th Ventricle Benign, cured by excision Extend of caudate or Septum into Lat Ventricle
Sheets or Rosettes Young>Old, Accounts for 1/3 of posterior fossa neoplasms Children = midline, young adults = lateral CSF Metastasis Invades leptomeninges & seeds CSF, Good prog except large cell Medulloblastoma Grows in sheets or rosettes Myc Amp & LOH 17p Bad = < 3yo, Mets, Large Cell Variant, Myc Amp, LOH 17p May Metastasize into CSF Retinal S, Rhodopsin, TrkC R Good = Retinal S Antigen, Rhodopsin & TrkC receptor Grows in sheets w/ poor cytoplasmic borders Women Rare in children, More common in adult women Whorls & Psammoma Bodies Attached to Dura Slight tendency to recur after excision Meningioma Vascular, Attached to dura, Benign Benign but Compress Brain Numerous Variants Hyperostic Rsponse Hyperostic Rsponse Bad = Clear Cell, Rhabdoid, Chordoid & Papillary Subtypes Encapsulated, Displaces, not Replaces nerves Encapsulated & Displaces Spindle = Antoni A (Verocay Bodies); Stellate = Antoni B Biphasic (Spindle & Stellate) Growth Pattern Female Intracranial Schwannoma Bilateral Acoustic Schwannomas = von Recklinghausen’s (NF I) CN VIII @ Cerebellopontine Angle or IAM CN VIII Also common in Neurofibromatosis Type II (NF II) CN V (less common) von Recklinghausen’s Encapsulated, Displaces, not Replaces nerves Biphasic (Spindle & Stellate) Growth Pattern Encapsulated & Displaces Spindle = Antoni A (Verocay Bodies); Stellate = Antoni B Intraspinal Schwannoma All Spinal levels Cystic 30% of spinal tumors Cystic
Encapsulated, Displaces, not Replaces nerves Encapsulated & Displaces Spindle = Antoni A (Verocay Bodies); Stellate = Antoni B Peripheral Schwannoma Biphasic (Spindle & Stellate) Growth Pattern von Recklinghausen’s Usually solitary, if multiple = von Recklinghausen’s
Arise from small peripheral nerves or trunks Replaces nerve Usually multiple, part of von Recklinghausen’s Neurofibroma Tumor mixed with collagen, reticulin & nerve Multiple Plexiform Neurofibroma = von Recklinghausen’s Hyperplasia of nerve supporting elements von Recklinghausen’s
Cerebellum, Retina, Medulla, Cervical Cord Men, Cerebellum Adult Male Predominance Supratentorial Meninges Foamy Cytoplasm Capillary Hemangioblastoma Lindau’s: Hemangioblastomas, Cysts, Adrenal/Renal Tumors Foamy Cytoplasm Erythropoietin Substance Add Retinal Angiomatosis = Von Hippel Lindau Syndrome Erythropoietin Substance→Polycythemia Lindau Syndrome
From Fibroblasts Primary Sarcoma Meninges, Perivascular, Choroid, Tela Choroidea Rare Attached to meninges CNS Pathology (Contd. 4) Disease Cause/Risk Factors Symptoms Buzzwords Other Diffuse Large B Cell Concentric Laminae Primary Lymphoma Diffuse Large B Cell Immunoblastic Reticulin Rare outside of immunosuppressed, Common in AIDS (Reticulum Cell Sarcoma) Diffuse Small B Cell Cleaved 9.5 B Cell Angiocentric growth, laminae, reticulin Suprasellar (Rathke’s Pouch) Children Most Common Supratentorial Tumor in children Solid or Cystic, Cords or Sheets (Epithelial) Hydrocephalus Often compresses Optic Chiasm or Hypothalamus Craniopharyngioma Keratin, Cholesterol Rich Cyst Fluid Keratin & Cyst Fluid May bulge into 3rd ventricle & compress CSF flow Rosenthal Fiber, Sharp Margins Rosenthal Fiber Slow growing, benign (difficult to irradicate due to islands) Most common in adult males Pineal or 3rd Ventricle Pineal or 3rd Ventricle Most common Germ Cell Tumor of CNS Germ Cell Neoplasms Males May Metastasize Same as Dysgerminoma/Sminoma, Embryonal Carcinoma, Metastasis Chorangiocarcinoma, Teratoma & Endodermal Sinus Tumor Skin Stratified Squamous Lining with Keratin Pons (Cerebello-Pontine Angle) Epidermoid Cyst Partially Calcified Rupture can cause Meningitis→Granuloma Keratin Pons (Cerebello-Pontine Angle) Calcified
Skin More Sebacious Glands Dermoid Cyst Sebacious “Cheese” Rupture can cause Meningitis→Granuloma Midline of Posterior Fossa Midline of Posterior Fossa
Rare in Cranium, more common in Spine Meningeal Metastasis Usually Multiple Hematogenous Seeding, Dissemination via CSF Most Common = Lung>Breast>Melanoma>Kidney>GI Tract (Metastatic Neoplasms to CNS) Spine May enter canal through Dural Root Sleeves
Usually Multiple Parenchymal Metastasis More common in Cerebrum than Cerebellum Cerebrum Most Common = Lung>Breast>Melanoma>Kidney>GI Tract (Metastatic Neoplasms to CNS) Lodge in grey matter at junction with white matter Grey Matter
Deficits occur & disappear completely; Important Predictor of Stroke Transient Ischemic Attack (if greater than 30-60 minutes causes infarction) (TIA) ½ of patients have a diffusion weighted MRI abnormality
Carotid,Vertebral, Basilar Atherosclerosis Middle>Posterior>Anterior Cerebral Arteries Stuttering Onset, at night Ischemic Necrosis; Most common of all CV Disease Age>60, Arteriorsclerosis (DM & HT) Vasodilation & Immediate Metabolic Change Older Patients & TIA 1-2d: loss of definition of grey & white, edema; 2-10d: demarcation Cerebral Infarction Inflammation, Compression, Spasm Acidosis; Edema; ↑ Glu; Ca2+ Influx; Free Radical Atherosclerosis >10d: liquefaction & cyst formation Polycythemia, Hypotension, ↓ O2 PMNs; c-fos, cjun & HSPs c-fos, cjun & HSPs Goal of focal ischemic stroke is to protect penumbra Heart Arrhythmias & MI Arrhythmias & MI Aorta & Carotid Plaques Middle Cerebral Artery Sudden Onset Fat emboli cause petichial hemorrhages in white matter of cerebrum Cerebral Embolus Endocarditis Lesions in cortex & corticomedullary junction Multiple Regions Change of “no flow/reflow” hemorrhage Surgery & Trauma Rapid Improvement (some) Charcot-Bouchard Aneurysms Hypertension Putamen & Pons = Death;Thalamus & Cerebellum = Recoverable Hypertension Disection of parenchyma, rupture into ventricles Waking Hours Cerebral Hemorrhage Older pts with amyloid can get lobar hemorrhage w/o hypertension Amyloid Hematoma ringed by petichiae 50% Coma High 30 day mortality Large amounts of hemosiderin after recovery Some stiff neck/headache Head Trauma Head Trauma (Saccular Aneurysm) Ruptured Aneurysms, Neoplasms Arterial Spasms & Cerebral Infarction Sudden Onset during Day Subarachnoid Hemorrhage Arteriovenous Malformations, Dyscrasias Hydrocephalus Headache & Stiff Neck in all Extension of Hemorrhage Younger Patients; Seizures CNS Pathology (Contd. 5) Disease Cause/Risk Factors Symptoms Buzzwords Other Fibrinoid necrosis Hyalinization of media & narrowing of lumen Lacunar Infarction Hypertension Small (< 1 cm) Grey Matter, Internal Capsule, Basis Pontis & Centra Semiovales
Mycotic Aneurism Bacterial Emboli Distal to bifurcation of Circle of Willis Cerebral Embolus Cause Subarachnoid & Intracerebral Hemorrhage
Found on penetrating intraparenchymal arteries Charcot-Bouchard Aneurysms Hypertension Cerebral Hemorrhage Microaneurysms Cerebral Hemispheres, Cerebellum & Brainstem
85% in anterior circulation Congenital Defect at Bifurcation Internal Carotid, Anterior Cerebral Berry Aneurysm Saccular Aneurysms Degeneration of IEL Subarachnoid Hemorrhage & Anterior Communicating Multiple in 20% of patients Atherosclerosis Hemorrhage or Compression
Vertenral, Basilar or Internal Carotid Fusiform Aneurysms Segmentally Dilated Don’t Rupture Compression
Pons or Cerebral White Matter Focal Seizures Capillary Telangiectasis Pons or Cerebral White Matter Small Dilated Capillaries separated by neural tissue Repeated Subarachnoid Hemorrhage Intracranial Bruits
Focal Seizures Cavernous Malformations Repeated Subarachnoid Hemorrhage Dilated Sinusoidal Vessels without neural tissue Intracranial Bruits
Found along Middle Cerebral Artery Focal Seizures Arteriovenous Malformation Middle Cerebral Artery Composed of arteries & Veins Repeated Subarachnoid Hemorrhage Intracranial Bruits Found over Subarachnoid Space over Cord Focal Seizures Large Numbers of Veins Venous Malformation Subarachnoid Space over Cord Repeated Subarachnoid Hemorrhage Intracranial Bruits Infection, Heart Disease, Post-op Trauma Superior Sagital Sinus or Superior Cerebral Veins Carcinoma, Fever, Dyscrasias, Hemorrhage into leptomeninges Venous Occlusive Disease Sinus or Veins Bad = If thrombosis spreads into bridging veins (don’t use TPA) Dehydration, Cachexia, Hypotension Hemorrhagic Infarction Puerperium Hemorrhage in cortex (white matter) Neonates: Group B Strep & E. coli Fever, Headache, Photophobia, Nuchal Rigidity A leptomeningitis (leptomeninges & subarachnoid CSF) ↓ Acute Pyogenic Meningitis <2 y: S. pneumoniae (H. influenza?) Change in mental status Glucose (CSF) With Treatment: Complete resolution or with mild impairment PMNs (Bacterial) >2 y: N. meningitides ↑ CSF Pressure, PMNs, Protein; ↓ Glucose Complications: Hydrocephaly, Infarct, Blindess, Deafness, Ocular Medical Emergency Elderly: S. pneumoniae & Listeria Hydrocephaly, Infarct, Seizures, CN Palsies Palsy, Seizures
Effects more mild than Bacterial Aseptic Meningitis Enterovirus ↑ Lymphocytes Usually self-limiting, no long term effects (Viral) (Echovirus, Coxsackie or Poliovirus) CSF Pressure, Lymphocytes, Protein CNS Pathology (Contd. 6) Disease Cause/Risk Factors Symptoms Buzzwords Other Less Fulminating than Bacterial ↑↑ Protein Meningoencephalitis (Meninges & Brain Parenchyma) Chronic Meningitis ↑ CSF Pressure, Mono’s or Mixed, Protein Mycobacteria (TB) Mononuclear Cell Very hard to treat, high rate of complications (Mycobacterial) Basal Meninges Basal Meninges CSF Protein may be very high with TB Granulomatous Reaction (not pyogenic) Candida Less Fulminating than Bacterial ↑↑ Protein Meningoencephalitis (Meninges & Brain Parenchyma) Chronic Meningitis Mucor (with Diabetic Ketoacidosis) ↑ CSF Pressure, Mono’s or Mixed, Protein Mononuclear Cell Very hard to treat, high rate of complications (Fungal) Aspergillus Basal Meninges AIDS & Diabetes CSF Protein may be very high with TB Cryptococcal (with AIDS) Granulomatous Reaction (not pyogenic) Basal Meninges Mucor & Aspergillus tend to invade blood vessels (hemorrhagic)
Bacteria (Staph & Strep) Herniation due to mass effect Predisposed: Endocarditis; Heart Disease; Brain Abscess Fungi (often immunodeficient) Rupture into ventricles Lung, Sinus & Tooth Infections Protozoa (Toxoplasma - AIDS)
Eastern Equine-Epidemic Viral Encephalitis Mononuclear Infiltrate, Microglial Nodules West Nile Epidemic Eastern Equine = most virulent, 20-40% mortality (Arbovirus) Neuronophagia, Viral Inclusion Bodies Western Equine
HSV-1 = Most common cause of sporadic acute encephalitis Viral Encephalitis Mononuclear Infiltrate, Microglial Nodules Labial Herpes not a significant risk factor HSV-1 Inferior Temporal & Frontal Lobes (Herpes Simplex Type I) Neuronophagia, Viral Inclusion Bodies Treatment = Acyclovir Tropism for Temporal & Frontal Lobes except in neonates (pan)
In immunodeficient pts & neonates; In others = aseptic meningitis Viral Encephalitis Mononuclear Infiltrate, Microglial Nodules HSV-2 High Risk = Babies born to mothers with active genital herpes (Herpes Simplex Type IIK) Neuronophagia, Viral Inclusion Bodies Neonates = generalized panencephalitis (no tropism) like above
Mononuclear Infiltrate, Microglial Nodules Viral Encephalitis Posterior Ganglionitis VZV Neuronophagia, Viral Inclusion Bodies Exemplifies latency (Varicella Zoster Virus) Latency Inflammation of a sensory ganglion
Peripheral Nervous System as route of entry Mononuclear Infiltrate, Microglial Nodules Viral Encephalitis Hyperexcitability (slowly spreads along peripheral nerves) Rabies Neuronophagia, Viral Inclusion Bodies (Rabies) Pharyngospasm Slight Touch: Pain,Violent Motor Response, Convulsions Hyperexcitability Swallowing: Pharyngospasm (fear of water)
Most common opportunistic virus infecting CNS in AIDS Viral Encephalitis Mononuclear Infiltrate, Microglial Nodules CMV Periventricular Succeptability in fetuses & immunodeficient (Cytomegalovirus) Neuronophagia, Viral Inclusion Bodies Periventricular localization
Mononuclear Infiltrate, Microglial Nodules Only immunodeficient individuals succeptable Progressive Multifocal Oligodendrocytes JC Virus Neuronophagia, Viral Inclusion Bodies Tropism for oligodendrocytes Leukoencephalopathy Loss of myelin Widespread loss of myelin Poor Prognosis
Mononuclear Infiltrate, Microglial Nodules Infected: Macrophages, Giant Cells Microglia (NOT neurons) Viral Encephalitis Neuronophagia, Viral Inclusion Bodies Can lead to: Toxo, CMV, Cryptomeningitis, PML HIV-1 Doesn’t Infect Neurons (HIV) Dementia, Ataxia, Incontinence, Seizures 2 most common focal lesions: Toxo Abscess & 1º Lymphoma Cerebral Atrophy, Ventriculomegaly Infection is rare in congenital AIDS
Absence of Deep Tendon Reflexes Meningovascular: Meningitis, Meningeal Arteritis Neurosyphilis Paretic: Invastion of parenchyma (dementia & motor instability) Treponema pallidum Charcot Joints (Tertiary Syphilis) Tabes Dorsalis: Destruction of Dorsal Roots (Ataxia, Skin & Joint “ Lightning Pains” Lesions[Charcot Joints], Dysesthesia, No deep tendon reflexes) CNS Pathology (Contd. 7) Disease Cause/Risk Factors Symptoms Buzzwords Other Meningitis Neuroborreliosis Encephalopathy Major arthropod born disease in US; Evolves through 3 stages Borrelia burgdorferi (Lyme Disease) Facial-nerve paralysis Nervous System involved in Stage 2 (months) & 3 (years) Polyneuropathies Prion (PrPSc) Dementia, Ataxia, Insomnia, Paraplegia Most Common is Sporadic = Creutzfield-Jakob Disease (CJD) Transmissible Spongiform Sporadic Paresthesias, Deviant Behavior PrPSc Infection: Corneal Transplants, Electrodes, Dural Grafts & GH Encephalopathy Genetic No Inflammation; Vacuolization of Tissue No Inflammation Course is relentlessly progressive, fatal in a year Infectious (Dementia & Startle Myoclonus = CJD) Head Trauma, Early Low Linguistic Skill Progressive decline in memory & cognitive fxn ½ of pts over 85 have AD APP, PS1,PS2 Low Educational Achievement Personality & Behavioral Changes Areas Affected: Basal Nucleus (Ach), Locus Ceruleus (NE) & Dorsal Alzheimer’s Disease Tau Tangles APO E-4 Neurofibrillary Tangles (Tau) & Plaques (A) Tegmentum (5HT); Entorhinal Cortex & Hippocampus APlaques APP(21), PS1, PS2 & Chr 10 Mutations Loss of CAT & Acetylcholineesterase Treatment: Cholinesterase Inhibitors, NMDA Antagonists & Vit. E Onset: Personality & Behavioral Changes Frontotemporal Dementia Inherited Impaired Judgement, Language & Memory Pick Bodies Pick Bodies = silver positive cytoplasmic inclusions (Pick’s Disease) Chr 17 & Tau gene mutations Frontal & Temporal Lobe Atrophy Chr 17 Pick Bodies, Balloon Cells Age, Tremor, Cogwheel Rigidity, Akinesia Substantia Nigra Mitochondrial Dysfunction Disturbances of Posture, Equilibrium & Locus Ceruleus Most Frequent Basal Ganglia Disorder Parkinson’s Disease Oxidative Stress Autonomic Funciton; Dementia Lewy Bodies 12 genetic mutations: PARK 1-10, NR4A2, Synphilin-1 Excitotoxicity, Toxins (MPTP) Substantia Nigra & Locus Ceruleus Damaged Loss of melanin & Dopamine
Dementia, Psychoitc Behavior, Parkinsonism Dementia with Lewy Bodies Second Most Common Dementia of Elderly Lewy Bodies, Senile Plaques, Tangles
Choreoathetoid Movement & Dementia Genetic (AD) GABAergic medium spiny striated neurons ↓ Genetic Test available for confirmation Huntington’s Disease GABA, Glu Decarboxylase, HD gene = Chr 4 p16.3 (36-121 CAGs) Atrophy of Caudate & Putamen CAT Patients have a high suicide rate Ventricular Enlargement & Frontal Lobe Atrophy Limb & Trunk Ataxia Most Common Inherited Ataxia Genetic (AR) Loss of limb proprioception & deep tendon reflex Friedreich’s Ataxia Small Spinal Cord Degeneration of posterior spinal cord Frataxin = 9q13-q21.1 (200-900 GAAs) Dysarthria & Extensor Plantar Response Frataxin = unknown function, but disease due to loss of function Kyphoscoliosis, Cardiomyopathy & DM
Genetic Spinocerebellar Ataxia Type I Second Most Common Triplet Repeats within gene
Dentato-rubro-pallido-luysian Genetic Atrophy Triplet Repeats within gene
Genetic Machado-Joseph Disease Triplet Repeats within gene
Excitotoxins, Viral Infection Upper & Lower Motor Neuron Degeneration More common in men; rapid progression toward death Immunological Abnormalities Lower: Atrophy, Fasiculations, No reflexes Upper & Lower Motor Neuron Familial ALS = Superoxide Dismutase gene on Chr 21 Amyotrophic Lateral Sclerosis Trace Elements & Free Radicals Upper: Hyperreflexia, spasticity No inflammatory reaction Difficulty swallowing & chewing; Cell loss most intense in cervical Genetic (10%) Chr 21 Demyelination & atrophy of anterior cord No inflammatory reaction CNS Pathology (Contd. 8) Disease Cause/Risk Factors Symptoms Buzzwords Other
Progressive Bulbar Palsy Brainstem Motor Nuclei Rapidly Progressive
Progressive Spinal Muscular Anterior Horn Cells & Nerve Root Anterior Horn No change in corticospinal tract Atrophy
Primary Lateral Sclerosis Corticospinal Tract Corticospinal Tract
ALS-Parkinsonism Dementia Complex of Guam