Report of the Incident Management Team into the Hepatitis C Look back in Gwynedd 2005-7 Executive Summary
In October 2005, the National Public Health Service for Wales (NPHS) was formally notified of a case of current Hepatitis C in a practising health care worker in the Gwynedd Local Health Board (LHB) area. An Incident Management team was established under the chairmanship of the Chief Executive of the Local Health Board to consider and investigate any public health consequences that may have arisen and to assure the safety of the patients who may have been treated by the health care worker.
The Incident Management Team carried out a risk assessment on the basis of the information gathered regarding the nature of the Hepatitis C infection, the type of heath care practice involved and the governance arrangements of the health care worker in relation to infection control. The Incident Management Team sought advice from the UK Advisory Panel for health care workers infected with Blood-borne Viruses (UKAP) on this risk assessment. UKAP advised that a Look Back should be carried out for Hepatitis C, Hepatitis B and HIV. The UKAP Toolkit for the management of Look Backs was obtained and modified for local use.
The Look Back involved an examination of 6,139 patient records and resulted in the identification of 5,054 exposed patients, 4,147 resident in North Wales and 907 outside the region. A helpline run by NHS Direct Wales for pre-test counselling was set up and 2,263 patients attended special clinics set in the local area, the rest being offered screening by their GPs. 2,665 patients were eventually tested for Hepatitis C, Hepatitis B and HIV.
The Incident Management Team found no evidence of anyone being infected with Hepatitis C by the health care worker. There was also no evidence of any patient infecting another patient with Hepatitis C, Hepatitis B or HIV during treatment by the health care worker. Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Glossary of terms and abbreviations
AM Assembly Member (of the National Assembly for Wales).
Analytical epidemiology
A study in which groups are compared to identify and quantify causes of disease by testing a theory as to what the cause may be. A case-control study is an example of an analytical epidemiological study.
BBV Blood-borne Virus. These are viruses which some people carry in their blood and which may cause severe disease in some people and few or no symptoms in others. The main blood-borne viruses are HBV, HCV and HIV.
Caldicott Principles.
The six Caldicott Principles must be adhered to when collecting, transferring, or generally working with personal-identifiable information. The principles are:
Justify the purpose for using information
Only use when absolutely necessary
Use the minimum that is required
Access should be on a strict need to know basis
Everyone must understand his/her responsibilities
Understand and comply with the law
CC County Council.
CDSC Communicable Disease Surveillance Centre. It is based in the National Public Health Service for Wales.
CI Confidence Interval – see description below.
Case A person with the disease or condition under investigation e.g. hepatitis C infection.
Case Control Study
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 3 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
An analytical epidemiological study. It involves comparing people with a disease (cases) to a similar group of people free from that disease (controls) and looking back to see whether they were exposed to a risk factor of interest e.g. a history of intravenous drug abuse. Different rates of exposure between cases and controls may point to the cause of the disease.
Chi square A statistical test that estimates the probability that an observed difference between the proportion of individuals exposed to a risk factor in two groups could have occurred by chance. The test produces a p value (see definition below). A p=0.05 indicates a 5% probability, or a 1 in 20 chance that the difference could have occurred as the result of random variation.
Confidence interval
A way of expressing, statistically, the certainty about the precision of the findings from a study. The 95% confidence interval represents the range of measurements, calculated from a study, within which people can be 95% certain that the true value lies.
Confirmed case A person who submitted a blood sample in which one of the Blood-borne viruses was identified.
Control In a case control study (see above), a person without the disease or condition under investigation.
DNA Deoxyribonucleic acid: the genetic material which controls heredity and is located in the cell nucleus.
Descriptive epidemiology
Describing the characteristics of cases, i.e. date of onset of illness, place of residence, age or sex.
EHO Environmental health officer.
Epidemiology The scientific study of the patterns, causes, and control of disease in groups of people.
Exeter System The administrative database which contains the details of patients registered with GP practices in N Wales
Genotyping The process by which the hepatitis C virus is identified as belonging to a specific genotype (variants in the genetic structure of the virus)
GP General medical practitioner.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 4 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
GPC Wales The General Practice Committee of the British Medical Association in Wales HBV Hepatitis B Virus. This is a blood-borne viral infection that can be prevented through vaccination. The hepatitis B virus (HBV) causes hepatitis (inflammation of the liver) and can also cause long-term liver damage. HCV Hepatitis C Virus. This is a blood-borne virus that can cause long-lasting infection and can lead to liver disease. HCW Health Care Worker HIV Human Immuno-deficiency Virus. This virus causes Acquired Immune Deficiency Syndrome (AIDS). HIV destroys the body's ability to fight infection by attacking the immune system. This results in infected individuals becoming susceptible to opportunistic infections. HPA Health Protection Agency. The Health Protection Agency (HPA) is an independent body that protects the health and well-being of the population. The Agency plays a critical role in protecting people from infectious diseases and in preventing harm when hazards involving chemicals, poisons or radiation occur.
HPT Health protection team. Health protection teams in Wales are part of the National Public Health Service for Wales.
IMT Incident Management Team
LHB Local Health Board. In Wales, LHBs are the statutory bodies responsible for improving the health and well-being of the population, and for the planning and commissioning of healthcare services.
MP Member of Parliament.
NHSDW NHS Direct Wales – the Wales 24 hour telephone and e-health information service, which provides information about health, illness and health services
NPHS National Public Health Service for Wales - provides the resources, information and advice to enable the Welsh Assembly Government, Health Commission Wales, Local Health Boards, Local Authorities and NHS Trusts to discharge their statutory public health functions.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 5 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
NSTS The NHS Strategic Tracing Service holds administration data (e.g. NHS GP patient registration, GP and practice details) for the whole of England and Wales
NWWT North West Wales NHS Trust – the local provider of acute and community healthcare services
OR Odds ratio – see below.
Odds Odds refers to the ratio of the number of individuals being exposed to a risk factor to the number not being exposed to that risk factor. If among 10 cases of hepatitis infection 7 had a history of intravenous drug abuse and 3 had not, the odds would be 7/3.
Odds ratio The odds of exposure of cases to a risk factor divided by the odds of exposure of controls. Used to measure statistical association in case control studies. An odds ratio of 1.0 means that there is no association between the illness and the exposure. A value greater than 1.0 means there is a positive association i.e. disease more likely in the exposed. A value less than 1.0 means there is a negative association.
P value P-values are calculated by statistical tests to estimate how likely it is that the associations observed between an exposure e.g. using intravenous drugs and an outcome e.g. hepatitis C infection, could have been due to chance alone. A p-value of 0.05 means, therefore, that there is a 1 in 20 probability that the different levels of illness between an exposed and an unexposed group occurred by chance alone (and hence a 19 in 20 chance that there is some other “real” explanation). The smaller the p- value the more likely the difference between the two groups is real.
RA Risk assessment.
RNA Ribonucleic acid: an organic acid concerned with the synthesis of proteins.
Seroprevalence The frequency of occurrence of antibody (present in the blood, etc, in response to infection) in a given population.
T-test A statistical test used to determine whether the mean of a particular measurement in each of two groups is statistically different from the other
UKAP UK Advisory Panel for Health Care Workers infected with Blood- borne Viruses.
Univariate analysis
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 6 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Univariate analysis explores one risk factor at a time in an epidemiological study. The association between each risk factor and the disease is investigated separately.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 7 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
1. Introduction
This is the final report of the Incident Management Team (IMT) convened to investigate the potential public health consequences of a confirmed case of hepatitis C in a health care worker in Gwynedd.
The report details the way the incident was managed by the agencies involved and the steps taken to assure the safety of the public health. It covers:
The background and risk assessments that led up to the decision to undertake a look back
The arrangements that were put in place to support patients throughout the process
The outcome of the epidemiological investigation that was carried out.
From the outset, the IMT undertook to preserve the anonymity of the healthcare worker concerned, and this is reflected in the wording of this report.
2. Background
In October 2005, the National Public Health Service for Wales (NPHS) was formally notified of a case of current Hepatitis C in a practising health care worker in the Gwynedd Local Health Board (LHB) area. An Incident Management team was established under the chairmanship of the Chief Executive of the Local Health Board to consider and investigate any public health consequences that may have arisen and to assure the safety of the patients who may have been treated by the health care worker.
The Incident Management Team carried out a risk assessment on the basis of the information gathered regarding the nature of the Hepatitis C infection, the type of heath care practise involved and the governance arrangements of the health care worker in relation to infection control.
The Incident Management Team sought advice from the UK Advisory Panel for health care workers infected with Blood-borne Viruses (UKAP) on this risk assessment. UKAP advised that a lookback should be carried out. The UKAP Toolkit for the management of lookback was obtained and modified for local use.
3. Initial issue
On 3rd October 2005, a positive result of current hepatitis C result was reported by the microbiologist /Consultant in Communicable Disease Control (CCDC) in Ysbyty Gwynedd Hospital to the Regional Director of Public Health. This related to a blood sample from a Gwynedd health care worker who was being investigated by his/her general medical practitioner for unspecified ill health. Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 8 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
The health care worker was advised, and agreed, to stop working immediately. S/he was referred by the GP to the Gastroenterologist at the local District General Hospital for further advice and assessment.
The health care worker worked in a primary care setting where there was no formal access to Occupational Health Services. So, the initial occupational and social history was obtained by the local Consultant in Communicable Diseases Control and the Gastrointestinal Specialist Nurse.
The Chief Executive of the Local Health Board was also informed, and a meeting took place on 5th October 2005 to discuss the necessary immediate action.
The actions included:
1. The LHB would review all the records that they held in relation to the health care worker’s practise
2. A mapping exercise of known Hepatitis C virus notifications would be carried out to determine the prevalence of Hepatitis C in the community and determine whether there was a greater than expected number of cases in the Gwynedd area
3. A full risk assessment report would be sent to the United Kingdom Advisory Panel to seek their advice on how to proceed
LHB files relating to the health care worker were reviewed by a Public Health specialist. These revealed that concerns had been raised in the past, through routine inspections and two written patient complaints, regarding the infection control procedures in the health care worker’s practice.
Mapping of known HCV cases across the Gwynedd LHB area did not demonstrate an excess in the locality surrounding the health care worker’s practice, and the distribution of the specific genotype was similar to that reported for Wales as a whole.
The risk assessment was submitted and advice formally requested from the United Kingdom Advisory Panel on 21st October 2005.
4. United Kingdom Advisory Panel advice
The case was considered by the United Kingdom Advisory Panel at its meeting in November, and advice was received by the Incident Management Team on 21st December 2005. In the light of the information supplied, the Panel’s advice was that
“ … all the XXXX’s patients should be contacted and offered testing for HIV, and hepatitis B and C.”
The United Kingdom Advisory Panel also advised that the health care worker should be reported to the relevant regulatory body.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 9 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Following confirmation in May of the health care worker’s negative Hepatitis B and HIV status, and the completion of a revised risk assessment, the Incident Management Team proposed that the lookback should be restricted to offering testing for Hepatitis C only. It was felt that this approach would be less disruptive/invasive for the patients involved, given that the risk of patient to patient transmission of a Blood-borne virus infection was very small. This proposal was discussed verbally with the United Kingdom Advisory Panel. However, further written communication from the United Kingdom Advisory Panel confirmed their previous advice that tests for all three viruses should be offered, given the previous concerns about the health care worker’s infection control practice.
The Incident Management Team, therefore, put in place a system to
1. Identify the patients at risk/exposed
2. Provide a supported system to offer testing for the three blood-borne viruses patients may have been exposed to
3. Ensure adequate laboratory support to analyse the results
4. Implement a comprehensive communications plan to support patients, their primary care teams and the general public
5. Methods for Patient identification
The Incident Management Team decided that, in the absence of any evidence from the health care worker’s history of when infection was acquired, it would be prudent to include all those for whom records were available.
The records made available to the Incident Management Team dated from 1969. The records were not computerised and were probably not a complete history as, over the years, some patient records had been destroyed (e.g. records relating to patients who had left the area or joined other practices).
It was impossible for the Incident Management Team to assess the extent to which the records made available represented a history of the health care worker’s practice. A total of 6,139 records were eventually made available to the Incident Management Team.
Given the reported limitations from other lookbacks associated with obtaining complete patient listings from central administrative sources, no attempt was made to use this route.
An electronic database of patients was created from the paper records made available by the health care worker and all patient personal details verified where possible by comparison with the NHS GP registration system (Exeter system). This verification process identified those patients still resident in North Wales and those who had died whilst resident in North Wales. Further tracing was carried out on patients not immediately identified via this system, using the National Strategic Tracing Service (NSTS) database, which records details of all patients registered with Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 10 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
GPs in England and Wales, and also indicates where patients have moved to Northern Ireland or Scotland, emigrated or joined UK Forces. A minimum dataset was defined for this stage of the exercise. A copy of the data collection instrument is included at Appendix 1.
In line with Caldicott principles, access to both the Exeter System and National Strategic Tracing Service was restricted to named and identified individual members of Local Health Board staff.
A short protocol for extracting the data from the patient records was designed. The process was as in Appendix 2.
A unique Lookback Identification number was allocated to each patient and this was used as the key identifier at each subsequent stage of the process.
The data collection exercise took 5 working weeks from Monday 27 th March 2006, until Friday 28th April.
6. Patient notification
6. 1 Patients resident in North Wales
For those 4147 patients resident in North Wales, the next stage required validation of the patient lists by their GPs in order to identify those patients for whom contact regarding this issue by letter was felt to be inappropriate. Reasons for this would include under 18s, recently deceased patients, recently bereaved, terminally ill, learning disabled or mentally ill patients, and also those already known to be HCV, HBV or HIV positive. Lists of their patients were emailed to each practice with the request that they identify anyone who
Should not be contacted at all
Would require a blood test to be taken by a community nurse, or
The Incident Management Team needed to discuss further with the GP.
The LHB offered support in terms of salaried GP time to take some surgery sessions for some of the practices to enable them time to go through the lists.
The mailing to patients was undertaken by establishing a working party of staff drawn from partner organisations to copy, fold and insert the letter and information sheet, then seal, label and frank the 4000+ letters on the 30th May 2006. There were several different groups requiring different letters, i.e:
Gwynedd residents (offering testing via clinic appointment) Gwynedd residents (offering alternative testing via their GP) Gwynedd residents (children) Other North Wales residents (offering testing via their GP)
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 11 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Letters were hand delivered by community nursing staff rather than being mailed to the four individuals who were under 18.
Each patient received a bilingual letter (Appendix 3), and a bilingual fact sheet regarding Hepatitis B, Hepatitis C and HIV (Appendix 4).
48 letters were returned undelivered, despite the fact that names and addresses had been matched and GP validation process had been completed.
6. 2 Patients resident outside of North Wales
Data on 907 patients identified on the Exeter System as resident outside the North Wales area were passed to the Communicable Disease Surveillance Centre (CDSC), NPHS. These included patients resident in other parts of Wales, and elsewhere in the UK, the Irish Republic and other overseas residents, including armed forces personnel.
Given the widespread dispersal of out of area patients, Health Protection Agency Regional Epidemiologists (REs) in England and Northern Ireland, Consultants in Health Protection Scotland (HPS) and the Tri-Forces Consultant in Communicable Disease Control were contacted and asked to assist in contacting patients last known to be resident in their region.
Given the disparity between existing regional protocols for an exercise of this nature, Regional Epidemiologists were asked to cascade via their local Health Protection Teams to: Verify the current addresses and GP’s of patients where only the Primary Care Trust or equivalent was known Contact the GP to validate that the patient was registered with them (ie. check address/still alive/no reason why the patient should not be contacted) Communicate information about the lookback to individual patients, together with arrangements for local advice and obtaining blood samples from those who wished to be tested Ensure that blood samples were sent directly to NPHS Microbiology, Bangor who were coordinating the microbiological investigation.
A summary of procedures detailing what each patient and GP should receive was prepared by the Communicable Disease Surveillance Centre and included in the Regional Epidemiologist’s information pack.
The Communicable Disease Surveillance Centre sent to each contact point (Regional Epidemiologists etc.), a pack, including lists of names of patients believed to be resident, or last resident, in that region, specimen patients’ letters, laboratory request forms (one for each patient) and associated Question and Answer Briefings. The Communicable Disease Surveillance Centre ensured that each laboratory request form had the patient’s name, date of birth and unique lookback number on the label, to be matched with individually addressed patient letters. Arrangements were in place to ensure that each patient should have received from their local Primary Care Trust: Patients’ letter Hepatitis B, Hepatitis C, HIV fact sheet Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 12 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Microbiology request form specific to that patient.
Each GP should receive: GP letter Copy of Patients’ letter Information for GP’s/Practices
Similar arrangements were made through the NPHS for out of area patients resident in other parts of Wales.
7. Pre-test counselling
NHS Direct Wales (NHSDW) agreed to provide pre-test counselling for patients. Members of the Incident Management Team worked alongside NHSDW staff to develop a flowchart and script for the call handling staff. All Health Information staff were used to man the bilingual helpline with support from Nurse Advisers and Call Handlers during peak periods.
Once callers had contacted the helpline, staff would:
Discuss the nature of the lookback and discuss Hepatitis C, Hepatitis B and HIV; Follow the agreed algorithm to assess whether the patient wished to proceed to pre-test counselling; Ascertain whether a home visit was required; Verify place of residence; Agree an appropriate clinic time and location with the patient.
The web development team within NHS Direct Wales developed an electronic booking system for staff to make the appointments. This could be accessed via the NHS Intranet by named LHB staff to allow them to check the patients booked for each session.
Callers were transferred to a counselling team set up in the NPHS for further in depth advice if necessary.
8. Testing
The choice of virology test was based on feasibility of testing, acceptability to patients, cost and validity. Salivary testing, blood spot and venous blood sampling were the three methods considered. Venous blood sampling was considered to be the only evaluated test performed in accredited laboratories and offering appropriate sensitivity and specificity, despite its logistical drawbacks. See Appendix 5.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 13 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
As the majority of patients were resident in one relatively rural geographical area a number of suitable locations from which to offer blood sampling were required. The choice of locations was decided through a formal Option Appraisal process. The appraisal was based on the assumption that the only activity that would occur at the venues was Taking a blood specimen Answering any outstanding questions the patient had following the telephone pre- test counselling (in the event, this was only required by phone and was provided by NPHS staff)
Options considered were: 1. Minor Injury Units at existing Trust hospitals/clinics in the area 2. Non-NHS premises such as a community centre and leisure centre in the area 3. General practice surgeries in the area 4. Mobile premises such as a portakabin or trailer supplied by National Blood Transfusion Service 5. A combination of these
Criteria used for the option appraisal included accessibility for patients, availability of staff/skills/resources, transportation of specimens, access out-of-hours, and potential disruption of existing services. The option selected was the use of community hospital / clinic facilities (Bron y Garth Community Hospital; Bryn Beryl Community Hospital; Blaenau Ffestiniog Memorial Hospital; Dolgellau Community Hospital and Porthmadog Clinic).
Appendix 5 provides further information on the testing procedure followed.
8.1 . Administrative support for testing
Once the clinic venues had been agreed, arrangements were made to ensure the following was in place:
1. A rota of administrative staff to provide the reception and clerical support for each of the clinics which were run from 5th June 2006 to 12th July 2006. There were 39 sessions in all.
2. Provision of necessary information for each clinic. This included:
A clinic list for each session; laboratory forms; blood specimen bottles; GP codes; pre-printed labels; patient information sheets; lost ID forms; blood sample collection boxes
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 14 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
3. Agreement of payment arrangements to enable administrative staff to work unsocial hours.
4. Agreement of the role of the member of administrative staff, ie:
Maintain confidentiality; Arrange for the timely collection of blood samples at the end of the clinic session; Greet and book in patients as they arrived; Confirm patient details; Complete laboratory form and sample label and check patient details are identical; Inform the patient of the procedure for obtaining test results
The clinic system was initially designed with sufficient capacity for all 4000+ patients to attend if required. The web links established between NHSDW and the LHB enabled the available capacity to be scaled down quickly, once the pattern of demand for testing was clear.
A total of 2263 patients eventually attended the clinics. Phlebotomy services were provided by the North West Wales NHS Trust. NPHS staff provided telephone back up throughout all clinics to ensure that any questions raised could be addressed immediately for those attending the clinics.
9. Communications
9. 1 Planning The Incident Management Team agreed a communications plan for the lookback. This was based on the following strategic principles:
Communications should be direct with the patients affected and healthcare professionals as far as possible Communications should be proactive Incident Management Team actions should be open Incident Management Team actions should be speedy Communications should be through ‘one voice’ – the NPHS Communications should be in English and Welsh
Proposed actions depended on whether the healthcare worker wished to be named or whether the Incident Management Team needed to maintain confidentiality. There were a number of discussions and meetings with the healthcare worker in which the options were discussed. In the end the healthcare worker stated that s/he did not wish to be named.
A holding press statement was prepared for the possibility of the media finding out about the lookback before all the communication plans were in place.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 15 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
9. 2 Breaking news
BBC Cymru Wales broke the story of the lookback. On being approached for comment, the Incident Management Team made representations to the BBC at a senior level asking for the story to be held back until all plans for communicating with patients and healthcare professionals had been enacted. It was explained that plans were well advanced for communicating directly with those affected but that a story in the media before that had happened would raise concerns with many more people who would not know whether they were affected or not.
After a number of discussions, BBC Cymru Wales rejected Incident Management Team representations and broadcast the story the following day. Although reports emphasised that risk levels were very low, unnecessary concern was created with many members of the public who subsequently found out they were unaffected.
9. 3 Communication with the healthcare worker
As planning progressed, one member of the Incident Management Team was nominated as the communication point with the healthcare worker and updates and reports on progress were given on a regular basis. Copies of the letters to patients were shown to the healthcare worker and comments made were taken on board.
The healthcare worker did not see the final copies of the patient letters before they were issued because the Royal Mail failed to deliver a recorded delivery package on time. The Royal Mail has apologised for this.
9. 4 Communication with patients
See section on Patient Notification (Section 6) for details of the letter, fact sheet and helpline details made available.
All patients are being written to at the conclusion of the exercise with details of the findings of the lookback (Appendix 6).
9.5 Communication with Health care professionals
The Incident Management Team wrote directly on a number of occasions to GPs, pharmacists and dentists in Gwynedd and further afield to advise them of its actions and plans. The North West Wales Trust was also asked to inform front line staff so that they could respond to basic questions (Appendix 6).
Senior Managers in North Wales LHBs and Trusts were also briefed on the lookback as the story was broken and when plans were enacted.
The Incident Management Team liaised with the Health Protection Agency which made contact with healthcare professionals and affected patients living in England.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 16 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
All these professionals are being written to at the conclusion of the work with details of the findings of the lookback.
9.6 Web sites
The NPHS web site included information on the lookback, the infections involved, a Questions and Answers briefing and daily updates on action being taken. Gwynedd LHB’s web site provided links to the same information.
Both web sites will feature the lookback findings when the lookback is concluded.
The NHS Direct Wales website also information on the lookback, the infections involved and the Questions and Answers briefing. It also signposted access to the NPHS website.
9.7 Opinion leaders
The Incident Management Team briefed Board members, Welsh Assembly Government officials and the relevant Community Health Council officials as the story was broken and when plans were enacted.
The Incident Management Team wrote to Assembly Members, Members of Parliament, Gwynedd County Councillors and community councils in Gwynedd when the story was broken and when plans were put into place (Appendix 6). AMs and MPs were sent copies of the media updates issued by the Incident Management Team.
All these people are being written to at the conclusion of the work with details of the findings of the lookback.
9.8 Media
A holding statement was sent to the BBC and other media when the story was broken.
A briefing was held for the media when the letters to patients were issued. The briefing was led by the Regional Director of Public Health for North Wales for the NPHS and the Chief Executive of Gwynedd Local Health Board.
The Incident Management Team issued updates on the take up of tests for as long as the media was showing interest.
In the weeks that followed the story being broken, the NPHS responded to many dozens of media enquiries and questions and gave many interviews to broadcasters in English and Welsh. All media interview opportunities were accepted to explain the lookback and reassure people of the low risks involved.
BBC Radio Cymru made a half hour documentary on the lookback with which the Incident Management Team cooperated.
A media briefing is being arranged to coincide with the conclusion of the lookback.
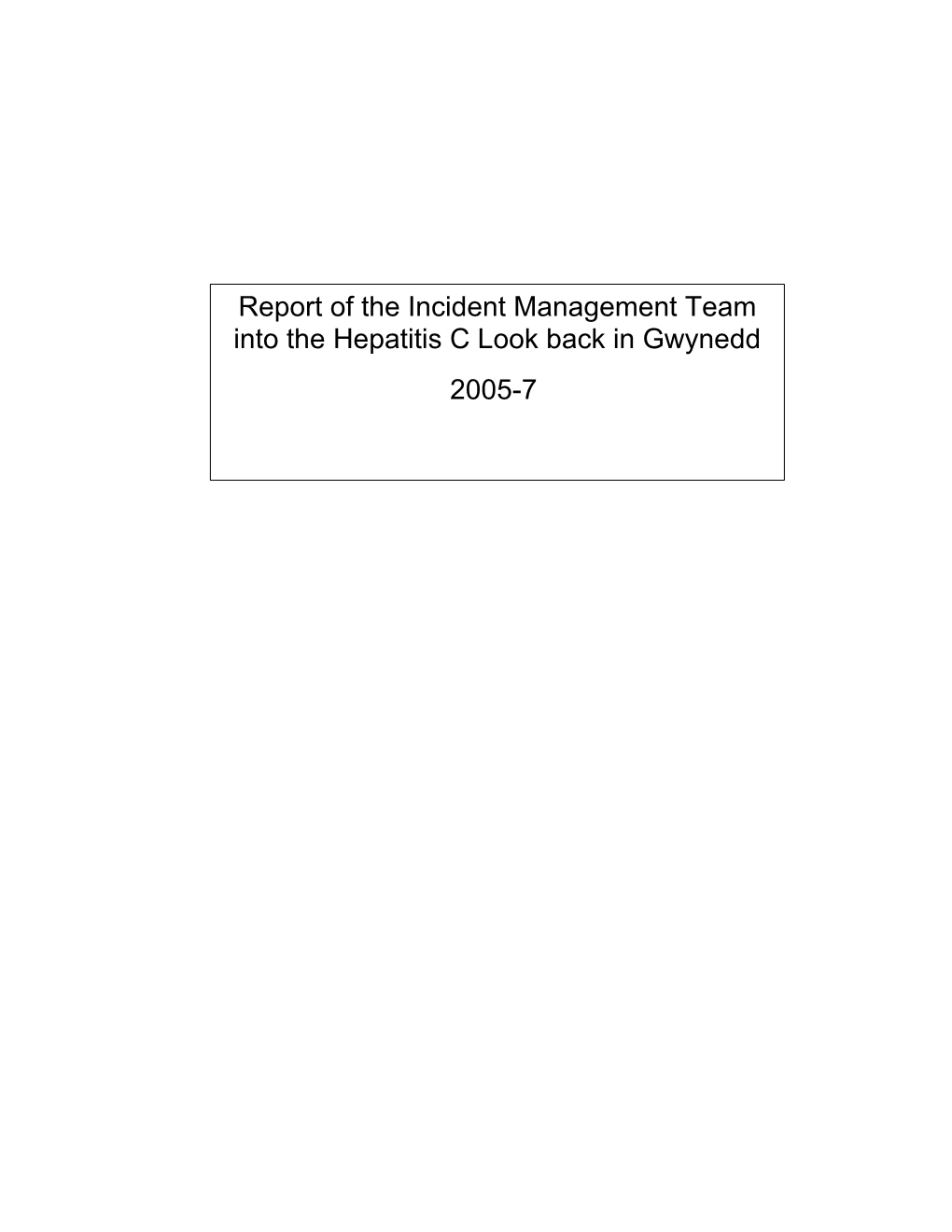
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 17 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report Total Records from Health Care 10. Results of notification exerciseWorker
Figure 1 shows how many patients6139 were traced and tested during the lookback 6139
Deceased Number Number not Identified traced
652 5054 433 Number identified
North Wales Outside North resident Wales 753
4147 907 Number not traced
Sent to GP for 154 validation
4147
Discuss further Community with GP Nurse visit OK to contact requested Do not contact
28 46
4033 40
28 Letters returned undeliverable Tested
48 2665
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 18 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
11. Outcomes from testing
11.1 Blood tests
A total of 2665 patients had blood tests.
Three weeks after the blood tests were obtained, patients with negative results resident in North Wales or out of area were able to obtain results via the NHS Direct Wales helpline.
In cases where there was a positive or equivocal test result and the laboratory request form was incomplete or GP contact details were unreadable, CDSC contacted Health Protection Teams to verify details of the patients’ GP. Positive and equivocal test results were communicated to patients by their GP, who also arranged appropriate clinical follow up by local services. Full details on how positive patients were followed up is given in Appendix 7.
Hepatitis C
11 patients tested positive for hepatitis C, indicating either past or current infection. Six of these patients were already known to be infected prior to the lookback. RNA genotyping was performed on eight of these patients.
One patient declined genotyping. Of the remaining ten, two were unsuitable for genotying due to absence of viral RNA. Of those genotyped, four patients had infection with genotype 1a, two with genotype 3a, one with genotype 2, and one had a mixed type of infection.
RNA sequencing was performed on seven patients plus the Health Care Worker (mixed infection makes it impossible to sequence the RNA). See Appendix 8 for a description.
None of the RNA sequences were shown to be related to each other (including that of the health care worker).
Hepatitis B
20 patients tested positive for hepatitis B. All of these were past rather than current infection.
HIV
Nine patients initially tested equivocal for HIV antibody. All were resolved as negative on subsequent testing.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 19 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
11.2 Clinical Patient Management
North Wales patients
Hepatitis C
North West Wales NHS Trust (NWWT) arranged extra clinics for patients tested as part of the lookback who tested positive for hepatitis C antibody. At these clinics, counselling was arranged, and blood was tested for circulating virus. These patients were then treated as any other patient with hepatitis C infection.
HIV
Nine patients with equivocal HIV antibody results were referred to the Genito-urinary medicine consultant at NWWT. On further testing, all proved negative.
Hepatitis B
Patients’ GPs were asked to take a sample of blood from patients who were hepatitis B core antibody positive and surface antigen negative, to confirm negative hepatitis B surface antigen status, and thus to provide evidence of a lack of current infection. All twenty proved negative, i.e. all had past rather than current infection.
Patients Resident Outside of North Wales
Patients testing positive for one or more of the blood-borne viruses were followed-up under local arrangements in their area of residence.
11.3 Epidemiology - prevalence of blood borne virus infection
The prevalence of hepatitis C infection in those tested was 0.41% (95% CI 0.21% - 0.74%). and the prevalence of past hepatitis B infection was 0.75% (95% CI 0.46% - 1.16%). These prevalences are at a level that would be expected in a population in this geographical area.
11.4 Case-control study
A total of 25 patients (eight patients with past or current hepatitis C infection, and 18 patients with past hepatitis B infection) were interviewed as part of the epidemiological study. One patient had been infected with both hepatitis B and C. Appendix 9 gives information on the case control study, letters sent to cases and controls and the consent form used and a detailed report on the study.
No association was found between blood-borne virus positivity and the amount or nature of treatment by the health care worker. Patients with past or current Hepatitis C infection were however significantly more likely to have used intravenous drugs that the controls.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 20 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
11.5 Interpretation of epidemiological and virology results
Transmission Hepatitis C from the health care worker to patients
The observed prevalence of hepatitis C virus infection of 0.41% (95% CI 0.21% - 0.74%) is similar to the estimated prevalence of hepatitis C virus in England of 0.5%. Seven of these eight cases of hepatitis C virus infection that agreed to be interviewed had other risk factors for hepatitis C infection.
Analytical epidemiology did not demonstrate any statistically significant association between treatment and infection with the hepatitis C virus. Sequencing of virus isolated from the two patients with same genotype as the health care worker demonstrated that the viruses were not related to the health care worker. The four patients from whom virus was unobtainable all had more likely alternative exposures to explain their hepatitis C virus infection.
There was no evidence which demonstrates transmission of the hepatitis C virus from the health care worker to a patient. The evidence available from patients who presented from testing suggests that this is unlikely to have occurred in this group of patients. These findings confirm the original risk assessment that the risk of transmission from the health care worker to a patient is low.
Transmission of Blood-borne virus from patient to patient
HIV
No patients tested positive for HIV infection and thus patient to patient transmission of HIV did not occur in the patients who were tested.
Hepatitis C
As discussed above the observed prevalence of hepatitis C virus infection was not elevated and the case-control study did not show any association between infection and the amount of treatment received.
Sequencing of virus isolated from the patients with the same genotypes demonstrated that the viruses were not related to each other. The four patients from whom virus was unobtainable all had risk factors for hepatitis C virus infection that were a more likely source than patient to patient treatment during treatment.
There is no evidence which demonstrates patient to patient transmission of the hepatitis C virus during treatment by the health care worker. The available evidence suggests that patient to patient transmission arising from any deficiency in infection control practice is unlikely to have occurred in the patients who were tested.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 21 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Hepatitis B
Data with which to compare the observed prevalence of past hepatitis B virus infection of 0.75% (95% CI 0.46% - 1.16%) is limited. However, the observed prevalence of anti-HBc in this investigation is at a level that might reasonable be expected.
Seven of these 18 cases who were interviewed had other high risk exposures for hepatitis B infection, and the remaining 11 had exposure that could have accounted for hepatitis B infection.
Analytical epidemiology did not demonstrate any statistically significant association between treatment and infection with the hepatitis B virus. No patients where found to have current infection with the hepatitis B virus and thus to have presented a risk to other patients for a prolonged period of time.
There is no evidence which demonstrates patient to patient transmission of the hepatitis B virus during treatment by the health care worker. The available evidence suggests that patient to patient transmission of the hepatitis B virus as a result of deficiency in infection control practice is unlikely to have occurred in the patients who were tested.
Conclusion: transmission of BBV from patient to patient
The initial risk assessment conducted by the NPHS concluded that the risk of patient to patient transmission of a blood-borne virus infection was probably very small but not zero. The assessment was reliant on there being a low prevalence of blood-borne virus infections in the relevant community rather than on the safety of the infection control procedures in operation.
Testing demonstrated that the assumption underpinning the initial risk assessment was correct. No cases of HIV or current hepatitis B infection were detected. Patients with evidence of past hepatitis B infection will have been infectious for relatively short periods of time in the past. It is not possible to date the onset of hepatitis B infection and thus determine if individuals were infectious at the time they received treatment.
The only patients who would have been infectious for longer periods of time and therefore likely to have presented a risk of transmission at the time when they were treated by the health care worker, were patients with current hepatitis C infection. Any deficiency in infection control practices during treatment of these patients had the potential to result in patient to patient transmission of the virus. In general terms the risk of transmission from patients with circulating virus in a healthcare setting is intermediate for hepatitis C between the higher risk for hepatitis B and lower risk for HIV. The patients with hepatitis C virus identified as part of this patient notification were unlikely to have acquired the infection as a result of treatment.
It is difficult to absolutely prove a negative. This would require all patients to present for testing and for virus to be recovered from all patients with evidence of blood-borne virus infection. Under half of the patients who were known to have been treated by the health care worker were tested. However, these findings confirm the original risk
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 22 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report assessment that the risk of transmission from the health care worker to a patient is low.
Appendix 10 gives a summary of the epidemiological investigation.
12. Discussion
12.1 Communications
The confidentiality of the healthcare worker as a patient was the most difficult issue to deal with from a communications perspective.
The following all called for the Incident Management Team to name the healthcare worker:
Some members of the public, who wanted to judge risk for themselves;
Some healthcare workers, who felt that they were being identified (wrongly) by their patients;
Some politicians and the media, who felt there was a public interest in doing so.
One media outlet – Golwg – published the name of what it believed to be the healthcare worker despite representations made to it.
There was also some concern expressed by politicians and health professional representative organisations about the pressures put on the healthcare worker. The need to look for hepatitis B and HIV were questioned in particular.
Undoubtedly, the lookback created pressures for the healthcare worker which were difficult for him/her to cope with. With the hindsight of the lookback’s conclusions perhaps people would not have demanded the name as they did.
The patient’s right to confidentiality is understood and respected. However, it would have been easier to communicate with patients, healthcare professionals and the public if the healthcare worker had wished to be named. It would probably have made it easier for the healthcare worker too.
The action proposed for people who self-identified as the healthcare worker’s patients – but whose names were not in the healthcare worker’s records – was another difficult communications issue.
The success of the Incident Management Team’s communications depended on understanding of risk. There was clearly much scope for alarm. Public understanding of hepatitis is low and fear is high. The prospect of catching infections from someone in the NHS is alarming because it challenges the reassuring perception of a safe NHS environment.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 23 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
An understanding of risk goes hand in hand with trust in those explaining the risk and an ability of individuals to understand (and control) the facts. The inability to name the healthcare worker inevitably undermined trust in the authorities and people’s ability to understand the facts. 12.2 NHS Direct Wales
Over 5,500 calls were answered by NHS Direct Wales (NHSDW) during the 35 weeks that the helpline was operating (12/5/06 to 22/1/07). Figure 2 shows a breakdown of these calls by week.
Calls Answered by NHS Direct 1800 1600 Patient letters sent 1400
s 1200 l
l Blood test results
a 1000 available c
. 800 o 600 N 400 200 0
Week ending
During periods of intense media coverage, in additional to handling patient calls, NHSDW staff fielded calls relating to the identity of the health professional involved, and captured information on 'self identifiers' and passed these details onto the Incident Management Team.
Health Information managers at NHS Direct Wales provided regular feedback to colleagues at the NPHS, clinics and Local Health Board on the level of activity and issues that needed to be addressed. Constant feedback on operational requirements was provided to all staff disciplines involved in delivering the helpline.
Although experience from some other lookbacks was available, it was difficult to predict with accuracy the level of involvement that would be required from NHS Direct, in terms of predicted call volumes, and timescales of the 0845 queries. This,
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 24 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report combined with the unpredicted breaking of the news earlier than hoped, and the magnitude of the numbers involved, presented a significant management challenge for NHDSW.
Some of the implications for the rest of the NHSDW service, particularly the challenge to redirect resources to front the helpline, may have been better understood had discussions begun earlier in the planning process.
12.3 Operational
Telephone conferencing
After two initial face to face meetings, all meetings of the Incident Management Team were conducted using telephone conferencing facilities. Members of the Incident Management Team were located in different settings across the length and breadth of Wales, and it would have been impossible to secure the required frequency of meetings in any other way. This proved to be an extremely time efficient and cost effective way of conducting the business of the Team. Simultaneous note-taking by the administrative officer supporting the Team allowed rapid turn round of action notes, and this again proved invaluable when the speed of events necessitated daily meetings.
Skill Mix and Multidisciplinary working
The range of different skills and knowledge required to managed an exercise of this nature cannot be over-emphasised. In addition to the wide range of specialist and technical Public Health / Microbiological / Virological support, it proved vitally important for the Team to have access to senior operational managers from the LHB and Trust who had the authority to quickly mobilise staff and resources. This facilitated the rapid implementation of plans which were in preparation when the news was broken earlier than anticipated.
Sound administrative management of a lookback is crucial, and the Incident Management Team was fortunate in the diligence of many members of staff from all the participating organisations who ensured that sound information governance principles were applied throughout, despite the complexity and magnitude of the exercise. Of particular note was the maintenance of the necessary confidentiality surrounding the early stages of the lookback.
12.4 Clinical Governance of the health care worker’s practice
This lookback was necessitated by concerns about the health care worker’s infection control practice. If these deficiencies had not occurred then there would not have been any significant risk of transmission of the hepatitis C virus from the health care worker to patients, and the patient notification exercise would not have been undertaken. These concerns also led to the risk of patient to patient transmission of BBV and the need to test for all three BBV as part of this lookback.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 25 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
At the time that these concerns were first recognised in the mid 1990s the health care worker provided emergency care for patients under NHS arrangements, but the majority of patients were treated privately. The Incident Management Team has asked Healthcare Inspectorate Wales to investigate the response by the NHS and other bodies to the concerns identified and how these were handled. The results of the investigation will be made public.
On the last occasion that the Health Authority attempted to address these concerns during 2002 the health care worker terminated their NHS contract and became fully private. The Health Authority, therefore, had no rights of inspection. The Health Authority asked the Health and Safety Executive (HSE) to investigate, but the HSE was unable to take on this work.
In due course, Healthcare Inspectorate Wales will report on the adequacy of the Health Authorities’ response prior to April 2002. However, between April 2002 and October 2005 the health care worker’s practice was in effect unregulated by the NHS. No effective statutory arrangements are currently in place for inspecting and investigating the provision of this aspect of private health care, although concerns about private practice are documented by the LHB and referred to the Health & Safety Executive or relevant professional body.
Appropriate legislation or regulations are required to give statutory responsibility for the regulation of this private health care activity to Healthcare Inspectorate Wales or another appropriate public body.
13. Learning for future lookbacks
The United Kingdom Advisory Panel toolkit recommends the identification of a senior, experienced individual to act as more or less full-time project manager for the duration of a lookback. This was not considered feasible in our case, and a number of individuals from the Incident Management Team were allocated responsibility for key areas. In the main this worked well, and a project management process was devised but as each of these individuals had many other responsibilities outside the lookback maintaining the momentum between meetings of the Incident Management Team was challenging.
For future lookbacks, the Incident Management Team would recommend to other teams that, if possible, one individual is released from other duties to co- ordinate the agreed project management framework.
There are, of course, significant benefits to having a number of individuals working on the different aspects of a lookback, especially as such events are relatively rare and so provide valuable training opportunities. However, our experience suggests that more dedicated co-ordination time early in the lookback may have been beneficial.
It is important for an Incident Management Team to establish at the outset a timetable for securing access to patient records. This should include a clear
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 26 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
process for understanding and using powers available for obtaining clinical records, and an appropriate timetable within which they should be retrieved.
Health care workers in some settings do not have routine access to Occupational Health services and this can present a challenge in the lookback situation, particularly in terms of ensuring advocacy and ongoing support for the health care worker. Contacts to a national clinician support service were provided to the health care worker in this lookback, but lack of expert occupational health service support did complicate some aspects if
NPHS The need to martial the NPHS resource across Wales at an early stage and to consider business continuity issues.
The need to coordinate the advice to be given to the Incident Management Team. This will prevent different advice being given by different NPHS professionals at different times.
Ensure that robust mechanisms are in place for patient notification of positive blood results.
LHB Workforce Implications The enormity of the workforce requirements for undertaking a similar lookback should not be underestimated. As events unfolded it became apparent that significant staff time would be necessary. Following the disclosure by the media it was necessary for Gwynedd LHB to put into practice its major incident plan to ensure that absolute priority was given to this work whilst at the same time ensuring that the immediate and essential functions of the LHB were fulfilled. The initial screening of patient data alone necessitated a core team of 8 personnel working full time for 5 weeks, in addition they were supported by over 60 other staff on an ad-hoc basis to process and validate the data as quickly as possible. This high volume of activity continued for several months with staff required to undertake a range of additional duties over and above their normal responsibilities. This included attending clinics seven days a week, working unsociable hours (early mornings, evenings and weekends), and dealing face to face and by telephone with patients who were understandably concerned.
Communication with GP practices Extensive efforts were made, as detailed in the communication plan to ensure that GPs were kept regularly informed of the progress of the lookback. Feedback locally and regionally indicates that this was successfully achieved. However, GPC Wales have identified that in future they would recommend that formal contact is made with GPC Wales to ensure general practice nationally is kept fully briefed.
Communication with Community Health Councils
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 27 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
It is important to note that effective communication between the LHB and the Community Health Council is imperative to ensure public confidence is maintained.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 28 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
13. Recommendations
Welsh Assembly Government should consider the points raised in the discussion and lessons learned (above)
Acknowledgements
The IMT would like to acknowledge the help they received from colleagues in the NPHS, Gwynedd LHB, North West Wales NHS Trust, Cardiff & Vale NHS Trust, NHS Direct Wales, the HPA, Business Services Centre, and UKAP.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 29 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Membership of the Incident Management Team
Grace Lewis Parry, Chief Executive, Gwynedd LHB (Chair)
Jo Charles, Associate Director of Public Health, NPHS/Gwynedd LHB
Dr Sandra Payne, Regional Director, NPHS/LPHD Gwynedd LHB
Kate Parry, Corporate Services Manager, Gwynedd LHB
Chris Lines, Head of Communications, NPHS
Dr Mark Walker, Consultant Microbiologist / Consultant in Communicable Disease Control (To end of May 2006)
Dr Chris Whiteside , Consultant in Communicable Disease Control, NPHS (from May 2006)
Dr Marion Lyons , Consultant in Communicable Diseases, NPHS
Dr Sandra Sandham, Director of Dental Public Health, NPHS
Dr Stuart Darcy, Consultant Microbiologist, NPHS (from May 2006)
Dr Rob Smith, Clinical Scientist, NPHS
Gary Porter-Jones, Public Health Nurse, NPHS
Dr Rob Atenstaedt, Specialist Registrar in Public Health, NPHS
Dr Roland Salmon, Consultant Epidemiologist, NPHS/CDSC Wales
Dr Brendan Mason, Consultant Epidemiologist, NPHS/CDSC Wales
Fiona Dennis, Health Information Services Development Manager, NHSDW
Leanne Hawker, Health Information Service Manager, NHSDW
Dr Nigel Waskett, Medical Director, NHSDW
Dr Fraser Campbell, Medical Director, Gwynedd LHB.
Dr Peju Famoriyo, Specialist Registrar in public health, NPHS
Rob Lewis, Directorate Manager for Community and Rehabilitation, North West Wales NHS Trust.
Teresa Owen, Specialist Trainee in public health, NPHS
Dr Tony Howard, Director for Infection and Communicable Disease, NPHS.
Lynne Chadburn, Personal Assistant, NPHS
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 30 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
APPENDICES
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 31 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 1 Data Collection Instrument
LOOKBACK REFERENCE _____ NHS Number ______
FIRST NAME (S) ______
SURNAME ______TITLE ______
OTHER RECORDED SURNAME ______
DATE OF BIRTH _____ / _____ / _____ DATE OF DEATH _____ / _____ / _____
Address on Record Address from Exeter system
Line 1 ______Line 1 ______
Line 2 ______Line 2 ______
Line 3 ______Line 3 ______
Line 4 ______Line 4 ______
DATE OF FIRST CONSULTATION ______/ ______/ ______
DATE OF MOST RECENT CONSULTATION ______/ ______/ ______TOTALPostcode NUMBER OF CONSULTATIONS ______Postcode ______
GP (from Exeter record) ______IF NOT N WALES RESIDENT
Telephone number PCT Code ______
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 32 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 2 Protocol for extracting data
1) Record data from the patient file on pre-numbered data collection form, thereby allocating each patient a unique identifier.
2) Check Patient name, date of birth and address details against Exeter system.
a) If positive match identified, complete additional details on data collection form.
b) If positive match not identified or Exeter system record suggests patient has moved, complete second search using National Strategic Tracing Service database
3) Transfer all information from completed data collection forms to Excel spreadsheet
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 33 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 3 Bilingual notification letter
Date as Postmark Private & Confidential
Dear Sir/Madam
I am writing to inform you that a healthcare worker who previously worked in Gwynedd has been found to have carried the hepatitis C virus. Our records show that you may have been cared for by this person.
The healthcare worker is no longer working.
I understand that this letter may cause you concern. However, the risk of a healthcare worker passing on the hepatitis C virus is very low indeed. It can only happen if the healthcare worker’s blood gets into the patient’s bloodstream.
As part of our work to assess the risk we have examined carefully the infection control procedures and records of the healthcare worker. This has raised concerns and we have sought advice from the United Kingdom Advisory Panel for Blood Borne Viruses. On this basis the Panel has also advised us that there is a very low risk of hepatitis B or HIV being passed on from one patient to another in the healthcare setting.
Although the risk to you is very small, I think it is important that you should be informed about the risk and given the opportunity to discuss the matter with qualified staff and to be offered a blood test. Your GP has also been informed in confidence about this matter.
If you would like to discuss the matter or book a blood test please call the special confidential contact line we have set up on 0845 6006086. Please have this letter to hand when you call. It will be staffed during the following times by people trained to answer your questions:
Monday to Friday 7 am to 8 pm
Saturday and Sunday 7 am to 4 pm
Although we have set up the line to cope with many calls, the line may be busy when you ring. Please do not hang up. Your call will be answered as soon as possible. If you hang up and try again, your call will go to the back of the queue.
The helpline staff will offer advice and support to help you decide whether you wish to be tested. Clinics will be held over the next few weeks, and include early morning, evening and weekend sessions. Please ensure that you take this letter with you when you attend to have your blood taken as the Reference number at the top of this letter will be required on the blood form Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 34 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
In view of the high number of patients involved, I regret it will not be possible for your GP surgery to take blood samples in this case.
The results of your blood test will be available 3 weeks after your test and you will be invited to telephone the helpline number for your results on the assumption that you do not have the infection. In the very unlikely event that we have a concern, I will ask your GP to contact you directly.
I do want to emphasise that the risk of you contracting hepatitis C, hepatitis B or HIV is very small indeed. I do understand that this letter may distress you, however, and I apologise if this is the case.
I enclose a fact sheet with more detailed information which you may find helpful and I do want you to know that we aim to respond to any concerns that you may have as quickly as possible.
Yours faithfully
Dr Sandra Payne Local Director of Public Health
Enclosure: Fact sheet
0845 6006086
PLEASE USE THIS SPACE TO RECORD THE DATE AND TIME OF YOUR CLINIC APPOINTMENT
DATE______
TIME ______
PLACE ______
YOUR RESULTS WILL BE AVAILABLE FROM THE HELPLINE NUMBER 3 WEEKS AFTER YOUR BLOOD TEST
DATE ______
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 35 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Dyddia fel marc y Post Preifat a Chyfrinachol
Annwyl Syr/Fadam
Ysgrifennaf i’ch hysbysu y canfuwyd fod gweithiwr gofal iechyd a oedd yn arfer gweithio yng Ngwynedd â’r firws hepatitis C. Mae ein cofnodion yn dangos efallai eich bod wedi derbyn gofal gan y person yma.
Nid yw’r gweithiwr gofal iechyd yn gweithio bellach.
Deallaf y gall y llythyr hwn achosi pryder i chi. Fodd bynnag, mae’r risg o weithiwr gofal iechyd yn trosglwyddo’r firws hepatitis C yn isel iawn. Gall ddigwydd os bydd gwaed y gweithiwr gofal iechyd yn cyrraedd llif gwaed y claf yn unig.
Fel rhan o’n gwaith i asesu’r risg, rydym wedi archwilio gweithdrefnau rheoli haint a chofnodion y gweithiwr gofal iechyd yn ofalus. Mae hyn wedi achosi pryder ac rydym wedi ceisio cyngor Panel Cynghori Firysau yn y Gwaed y Deyrnas Unedig. Ar y sail hwn, mae’r Panel hefyd wedi ein cynghori bod y risg o drosglwyddo hepatitis B neu HIV o un claf i un arall o fewn sefydliad gofal iechyd yn isel iawn.
Er bod y risg i chi yn fach iawn, rwyn meddwl ei bod yn bwysig y dylid eich hysbysu am y risg a rhoi cyfle i chi drafod y mater gyda staff cymwys a chael cynnig prawf gwaed. Hysbyswyd eich meddyg teulu am y mater hwn hefyd yn gyfrinachol.
Os hoffech drafod y mater neu drefnu prawf gwaed, gallwch gysylltu â’r llinell gyswllt gyfrinachol arbennig ar 0845 6006086. Gwnewch yn siŵr fod y llythyr hwn gerllaw pan fyddwch yn ffonio. Bydd yn cael ei staffio yn ystod yr amseroedd canlynol gan bobl a hyfforddwyd i ateb eich cwestiynau:
Dydd Llun i ddydd Gwener 7 am i 8 pm
Dydd Sadwrn a dydd Sul 7 am i 4 pm
Er y sefydlwyd y llinell ffôn i ymdopi gyda nifer o alwadau, mae’n bosibl y bydd y llinell yn brysur pan fyddwch yn ffonio. Peidiwch â rhoi’r ffôn i lawr. Atebir eich galwad gynted â phosibl. Os byddwch yn rhoi’r ffôn i lawr ac yn ffonio eto, bydd eich galwad yn mynd i ddiwedd y ciw.
Bydd staff y llinell gymorth yn cynnig cyngor a chefnogaeth i’ch helpu i benderfynu a ydych yn dymuno derbyn prawf. Cynhelir clinigau yn ystod yr wythnosau nesaf a byddant yn cynnwys sesiynau ben bore, min nos a phenwythnos. Sicrhewch fod y llythyr hwn gennych pan fyddwch yn mynd i gael prawf gwaed gan y bydd angen y Cyfeir-rif ar ddechrau’r llythyr hwn ar y ffurflen gwaed.
Oherwydd y nifer uchel o gleifion, yn anffodus ni fydd yn bosibl i’r feddygfa gymryd profion gwaed yn yr achos yma.
Bydd canlyniadau’r prawf gwaed ar gael 3 wythnos ar ôl y prawf a gwahoddir chi i ffonio’r rhif llinell gymorth ar gyfer canlyniadau gan gymryd na fyddwch wedi eich Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 36 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report heintio. Os bydd gennym bryder mewn achosion annhebygol iawn, byddaf yn gofyn i’r meddyg teulu gysylltu â chi yn uniongyrchol.
Hoffwn bwysleisio bod y risg i chi ddal hepatitis C, hepatitis B neu HIV yn isel iawn. Fodd bynnag, deallaf y gall y llythyr hwn achosi gofid i chi, ac ymddiheuraf am hynny.
Amgaeaf daflen ffeithiau gyda mwy o wybodaeth a all fod yn ddefnyddiol a hoffwn eich hysbysu y byddwn yn anelu i ymateb i unrhyw bryderon sydd gennych gynted â phosibl.
Yn gywir
Dr Sandra Payne Cyfarwyddwr Iechyd y Cyhoedd Lleol
Atodiadau: Taflen ffeithiau
0845 6006086 DEFNYDDIWCH Y BWLCH YMA I GOFNODI DYDDIAD AC AMSER EICH APWYNTIAD YN Y CLINIG
DYDDIAD______
AMSER ______
LLEOLIAD______
BYDD EICH CANLYNIADAU AR GAEL TRWY FFONIO’R LLINELL GYMORTH 3 WYTHNOS AR ÔL Y PRAWF GWAED
DYDDIAD______
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 37 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 4 Bilingual fact sheet.
Taflen ffeithiau Hepatitis B, Hepatitis C a HIV
Hepatitis B Hepatitis C HIV
Beth yw …? Mae’r firws hepatitis B yn achosi Mae haint hepatitis C yn firws a all Mae HIV yn golygu Firws Diffyg hepatitis (llid yr iau) a gall achosi niwed achosi haint hir barhaol a gall arwain at Imiwnedd Dynol ac mae’n firws yn y tymor hir i’r iau hefyd. glefyd yr iau. gwaed sy’n ymosod y system imiwn.
Pa mor gyffredin Amcangyfrifir bod 1 mewn 300 o bobl Mae hepatitis C yn haint prin – Dyma’r lleiaf cyffredin o’r firysau hyn – ydyw? wedi dal y firws yng Nghymru. amcangyfrifir bod 1 mewn 200 o bobl amcangyfrifir bod 1 mewn 4000 o bobl yn cario’r firws hwn yng Nghymru. yng Nghymru yn derbyn gofal ar gyfer HIV.
Sut mae pobl yn Mae heintiau’n digwydd trwy: Mae heintiau’n digwydd trwy: Mae heintiau’n digwydd trwy: cael eu heintio? Waed wedi’i heintio yn cyrraedd llif Waed wedi’i heintio yn cyrraedd llif Drosglwyddo hylif y corff (fel gwaed, gwaed rhywun arall gwaed rhywun arall semen, hylif o wddf y groth merch a Rhyw heb amddiffyniad gyda pherson Rhyw heb amddiffyniad gyda pherson llaeth y fron) heintus heintus er bod hyn yn brin iawn Rhyw heb amddiffyniad gyda phartner Gall y firws drosglwyddo o fam heintus Gall y firws drosglwyddo o fam heintus heintus i faban yn ystod beichiogrwydd, yn i faban yn ystod beichiogrwydd, yn Gall y firws drosglwyddo o fam heintus ystod genedigaeth neu yn dilyn ystod genedigaeth neu yn dilyn i faban yn ystod beichiogrwydd, yn genedigaeth. Ers Ebrill 2000, mae pob genedigaeth (6% o risg) ystod genedigaeth neu yn dilyn
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 38 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
gwraig feichiog yn y Deyrnas Unedig genedigaeth. Ers Ebrill 2001, mae pob yn cael cynnig prawf ar gyfer hepatitis gwraig feichiog yn y Deyrnas Unedig B. yn cael cynnig prawf HIV. Mae hepatitis C yn berygl galwedigaethol ymysg gweithwyr deintyddol a meddygol.
. Mae’n cymryd rhwng 6 wythnos a 6 mis Faint mae’n ei Yn aml, nid yw plant yn cyflwyno Mae’n cymryd rhwng 6 wythnos a 3 mis i ddangos bod y firws yn bresennol o’r gymryd cyn mynd unrhyw symptomau. Mae oedolion sy’n i ddangos bod y firws yn bresennol o’r adeg heintio, er yn aml mae’n cymryd yn sâl? dal y firws fel arfer yn sâl o fewn 6 mis. adeg heintio, er yn aml mae’n cymryd nifer o flynyddoedd cyn i symptomau nifer o flynyddoedd cyn i symptomau ddatblygu. ddatblygu. Hepatitis B Hepatitis C HIV
Mae haint hepatitis C yn effeithio ar Beth yw’r Nid oes gan lawer o bobl unrhyw Nid oes gan bobl gyda HIV symptomau wahanol bobl mewn gwahanol ffyrdd; arwyddion? symptomau, tra bod eraill yn dioddef am gyfnod maith, tra bod y firws yn nid yw llawer yn cael unrhyw salwch tebyg i’r ffliw gan gynnwys dolur gweithio’n araf i wanhau system imiwn symptomau tra bod eraill yn dioddef gwddf, blinder, poen yn y cymalau a y corff. Pan fydd system imiwn blinder difrifol ac yn gallu teimlo’n sâl diffyg chwant bwyd. Gall symptomau rhywun wedi gwanhau, bydd ef/hi yn iawn. Mae symptomau’n cynnwys eraill gynnwys teimlo’n sâl a chyfogi. agored i salwch arall, yn arbennig blinder, colli pwysau, teimlo’n sâl, Gall haint dwys fod yn ddifrifol gan heintiau (e.e. twbercwlosis a niwmonia) symptomau tebyg i’r ffliw, problemau achosi poen yn y bol a’r clefyd melyn a chanserau, nid yw nifer ohonynt yn canolbwyntio, poen bol a’r clefyd arfer bod yn fygythiad i berson iach. melyn.
Bydd 90% o bobl yn clirio’r firws yn Amcangyfrifir bod tua 15-30% o bobl dilyn haint mewn oedolyn. I’r gweddill, sydd wedi eu heintio yn clirio’r haint yn mae hepatitis B yn haint cronig a all fod naturiol o fewn 6 mis cyntaf ar ôl eu dros gyfnod o sawl degawd ac am oes. heintio. I’r gweddill, mae hepatitis C yn
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 39 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
haint cronig a all ymestyn dros gyfnod o sawl degawd ac am oes.
Sut fyddai rhywun Cynhelir diagnosis trwy brawf gwaed. Cynhelir diagnosis trwy brawf gwaed. yn gwybod eu bod Gan nad oes gan nifer o bobl unrhyw Cynhelir diagnosis trwy brawf gwaed. Gan nad oes gan nifer o bobl unrhyw wedi eu heintio? symptomau, mae’n bwysig cael prawf Gan nad oes gan nifer o bobl unrhyw symptomau yn ystod camau cyntaf o’r gwaed os byddwch yn teimlo eich bod symptomau, mae’n bwysig cael prawf haint, mae’n bwysig cael prawf gwaed mewn risg. gwaed os byddwch yn teimlo eich bod os byddwch yn teimlo eich bod mewn mewn risg. risg.
A oes triniaeth ar Mae brechlyn ar gael i atal pobl rhag Nid oes brechlyn ar gael i atal hepatitis Mae triniaeth effeithiol ar gyfer HIV. gael? cael hepatitis B. C. Mae triniaeth effeithiol ar gael i gleifion gyda hepatitis C. Mae triniaeth effeithiol ar gael i unrhyw un gyda hepatitis B.
Beth fydd yn digwydd os byddaf Mae unigolion positif yn cael eu Mae unigolion positif yn cael eu Mae unigolion positif yn cael eu yn bositif? hatgyfeirio i arbenigwyr ar gyfer hatgyfeirio i arbenigwyr ar gyfer hatgyfeirio i arbenigwyr ar gyfer triniaeth. triniaeth. triniaeth.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 40 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Hepatitis B, Hepatitis C and HIV fact sheet
Hepatitis B Hepatitis C HIV
What is …? The hepatitis B virus causes hepatitis Hepatitis C infection is a virus that can HIV stands for Human (inflammation of the liver) and can also cause long-lasting infection and can Immunodeficiency Virus and is a blood cause long term liver damage. lead to liver disease. borne virus that attacks the immune system.
How common is it? It is estimated that in Wales 1 in 300 Hepatitis C is a rare infection – there is This is the least common of these people have had the virus. an estimated 1 in 200 people carrying viruses – there is an estimated 1 in this virus in Wales. 4000 people in Wales being cared for HIV.
How do people get Infection occurs through: Infection occurs through: Infection occurs through: infected? Infected blood entering the Infected blood entering the The transfer of body fluids (such as bloodstream of another person bloodstream of another person blood, semen, fluid from the woman’s Unprotected sex with an infected Unprotected sex with an infected cervix and breast milk) from an person person although this is extremely rare infected person to an uninfected The virus can pass from an infected The virus can pass from an infected person. mother to child during pregnancy, mother to child during pregnancy, Unprotected sexual intercourse with when giving birth or after birth. Since when giving birth or after birth (6% an infected partner. April 2000, all pregnant women in the risk). The virus can pass from an infected
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 41 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
UK are offered testing for hepatitis B. mother to child during pregnancy, Hepatitis C is an occupational hazard in when giving birth or after birth. Since the dental and medical professions. April 2001, all pregnant women in the UK are offered tested for HIV.
It takes between 6 weeks and 6 months How long does it Children may often present with no It takes between 6 weeks and 3 months to show that the virus is present from take to become ill? symptoms. Adults who pick up the virus to show that the virus is present from when it was picked up, although it is are usually ill within 6 months. when it was picked up, although it is usually many years before symptoms usually many years before symptoms develop. develop. Hepatitis B Hepatitis C HIV
Hepatitis C infection affects different What are the signs? Many people have no symptoms while People with HIV usually have no people in different ways; many others experience a flu-like illness symptoms for a prolonged period of experience no symptoms at all while including a sore throat, tiredness, joint time, while the virus acts slowly to others experience extreme tiredness pains, and a loss of appetite. Other weaken the body’s immune system. and can feel very unwell. Reported symptoms may include nausea and When a person’s immune system has symptoms include fatigue, weight loss, vomiting. Acute infection can be severe been broken down, he or she is nausea, 'flu like symptoms, problems causing abdominal discomfort and susceptible to other illnesses, concentrating, abdominal pain and jaundice. especially infections (e.g tuberculosis jaundice. and pneumonia) and cancers, many of which are not normally a threat to a It is estimated that around 15-30% of healthy person. 90% of people will clear the virus after infected people clear their infections infection in adult life. For the remainder, naturally within the first 6 months of hepatitis B is a chronic infection that infection. For the remainder, hepatitis C can span several decades and can be is a chronic infection that can span life-long. several decades and can be life-long.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 42 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
How would Diagnosis is made by a blood test. As Diagnosis is made by a blood test. As Diagnosis is made by a blood test. As someone know if many people do not have any many people do not have any many people do not have any they were infected? symptoms, it is important to have a symptoms, it is important to have a symptoms in the early stages of blood test if you feel you have been put blood test if you feel you have been put infection it is important to have a blood at risk. at risk. test if you feel you have been put at risk.
Is there treatment There is a vaccination available to There is no vaccination available to There is effective treatment for HIV. available? prevent people getting hepatitis B. prevent hepatitis C. There is effective treatment available to patients with There is effective treatment available hepatitis C. for someone with hepatitis B.
What happens if I Positive individuals are referred to am positive? Positive individuals are referred to specialists for treatment care. Positive individuals are referred to specialists for treatment care. specialists for treatment care.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 43 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 5 Blood testing procedure
Choice of test Salivary tests do not offer appropriate levels of sensitivity and specificity for diagnostic purposes. There is evidence that blood spot testing may offer appropriate degrees of sensitivity and specificity for diagnostic purposes, but this method of testing has not yet been evaluated for this purpose. Venous blood sample testing is an evaluated diagnostic test performed in a laboratory having accreditation to perform that test. It offers appropriate levels of specificity and sensitivity, which are particularly important in diagnosing exposure to hepatitis C in low prevalence populations. However the test may be less acceptable to patients, requires phlebotomy skills, and samples would have to be transported daily to Ysbyty Gwynedd microbiology laboratory.
Collection of blood samples
Clotted blood samples were obtained as described above, and sent to the NPHS Microbiology Bangor laboratory in the North West Wales Trust (NWWT). Patient details were entered into the Laboratory Information Management System (LIMS) to create a report template. Samples and request forms were then forwarded on to the virology reference unit in Cardiff. Where so requested, the virology unit tested samples for Hepatitis B surface antigen and core antibody, Hepatitis C antibody and for HIV. Further samples of clotted and whole (EDTA) blood were requested from patients with equivocal results, in order to resolve the equivocal status. Samples of clotted and whole (EDTA) blood were also requested from patients with positive hepatitis C antibody results, to confirm the result, to demonstrate if infection was still present and to determine the genotype of any current infection. Further samples of clotted and whole (EDTA) blood were also requested from patients with positive Hepatitis B core antibody and negative Hepatitis B surface antigen results, to confirm their negative Hepatitis B surface antigen status.
Data collection
Blood results were then electronically transferred to the NPHS microbiology dept at North West Wales Trust (NWWT) where reports were generated and sent out to GPs. Negative results were compiled onto an Excel database. This database was updated weekly and was initially physically handed to NHSD Wales on a floppy disc, and later transferred by ftp from the NPHS Microbiology Bangor server, to the NHSD Wales server.
Positive and equivocal results were emailed by the microbiologist via secure server on a daily basis to the CCDC at the North Wales Health Protection Team.
The Health Protection Team collated the data for those patients who tested positive or equivocal for each of the three viruses. This included follow-up tests for the viruses and interviews for the case-control study (see Appendix 7).
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 44 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 6 Letters
6a Letter regarding the patient notification
An example is given below of the core text used in letters which were sent to
1. CHCs, AMs, MPs, Party health spokespeople, Gwynedd County Councillors, Gwynedd community councillors
2. Dentists, GPs (if any do not have patients on their lists), community pharmacists and other front line staff (c/o their Trust, LHB)
Dear
Look Back update
We are sending letters to 5,000 patients whom we believe have been cared for by a healthcare worker who previously worked in Gwynedd and who has been found to have carried the hepatitis C virus.
The healthcare worker is no longer working.
I understand that these letters may cause concern. However, the risk of a healthcare worker passing on the hepatitis C virus is very low indeed. It can only happen if the healthcare worker’s blood gets into the patient’s bloodstream.
In line with national guidelines, as part of our work to assess the risk, we have examined carefully the infection control procedures and records of the healthcare worker. This has raised concerns and we have sought advice from the United Kingdom Advisory Panel for Blood Borne Viruses (UKAP). On this basis the Panel has also advised us that there is a very low risk of hepatitis B or HIV being passed on from one patient to another in the healthcare setting.
Advice, support and testing
Although the risk to patients is very small, I think it is important that patients should be informed about the risk and given the opportunity to discuss the matter with qualified staff and to be offered a blood test.
For patients who would like to discuss the matter or book a blood test we have set up a special confidential contact line. It will be staffed during the following times by people trained to answer their questions:
Monday to Friday 7 am to 8 pm
Saturday and Sunday 7 am to 4 pm
The helpline staff will answer any questions patients may have and offer counselling to help people decide whether they wish to be tested.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 45 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
We have put in place a programme of 47 clinics for blood testing in the areas where most of the patients live. There are clinics set up in the morning, afternoons and evenings and at weekends. For people who no longer live in the area, we have made arrangements for their GPs to organise the blood tests.
The blood test results will be available three weeks after the test and patients will be invited to telephone the helpline number for their results on the assumption that they do not have the infection. In the very unlikely event that we have a concern, we will ask the patient’s GP to make contact directly to discuss the concern.
It is possible that some patients will identify themselves at risk on the basis of rumour or media reports about the name of the healthcare worker. I wish to stress that the look back is concerned at this stage with those individuals for whom we have healthcare records. Currently, we have no evidence to suggest that any individual has suffered ill health as a consequence of having care provided by the healthcare worker.
When this look back is completed, we will reassess the risk, supported by UKAP, and, if it changes, we will consider what public health action will be required for those for whom we may not have a health record.
GPs, of course, may offer a blood test to a patient on the basis of the symptoms they present or other risks that the patient may identify.
Infection control procedures
Our review of the healthcare worker’s infection control procedures and records raised concerns as I have said. It is apparent from our records that concerns about infection control procedures have been raised with health authorities in the past. I have therefore asked Healthcare Inspectorate Wales to investigate the response by the NHS and other bodies to the concerns raised and how these were handled. The results of the investigation will be made public.
The work of the Incident Management Team
I also enclose a timeline for the incident, explaining the process which has brought us to this point. It has taken much time and effort to respond to the healthcare worker’s diagnosis, involving the following work:
Detailed examination of the risk to patients including an examination of the healthcare worker’s infection control procedures and history;
Detailed examination of more than 5,000 patient records going back more than 30 years, checking the accuracy of the addresses, noting changes of address, noting patient ages (to allow appropriate contact with children) and noting GP details;
Building a database of patients to be contacted;
Drafting of correspondence with patients according to residence and age; and to their GPs;
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 46 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Establishment of an advice line staffed to provide advice and support and to book appointments for 5,000 patients bilingually and with an anticipated surge of activity in a short period;
Establishment of clinics with staffing to arrange blood tests for every patient who asks for one;
Establishment of arrangements for patients to have a blood test taken by their GP if they have moved away;
Establishment of laboratory facilities and systems to manage the substantially increased demand for blood testing;
Translation of all communication material into Welsh;
Verification of the patient details, and the appropriateness of an approach by letter, from each of their GPs.
You will appreciate that this has been a massive exercise. More than 100 NHS staff are involved.
In all that we have done, we have placed the highest importance on doing the right thing – taking advice from experts, learning from previous Look Backs, and making sure that we only contact the right people in the most sensitive way.
Patient confidentiality
Some people have asked why the name of the healthcare worker has been kept confidential. The healthcare worker, like any patient, has a right to confidentiality. This is very important for the person concerned. It is also important if we are to expect healthcare workers to be open and to co-operate fully with the NHS in future such cases of infection.
It is quite possible – and has been the experience elsewhere – to conduct a Look Back of patients without compromising the confidentiality of the healthcare worker.
We have given the healthcare worker the opportunity to put his/her name in the public domain but s/he has decided not to do so as is his/her right.
In maintaining the healthcare worker’s confidentiality, we have taken into account an assessment of the risk to patients. The risk of a healthcare worker passing on the hepatitis C virus to a patient is very low indeed.
Further information
I do want to emphasise that the risk of patients contracting hepatitis C, hepatitis B or HIV is very small indeed.
I enclose a fact sheet with more detailed information which you may find helpful and I do want you to know that we aim to respond to any concerns that people may have as quickly as possible.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 47 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
If you have any issues you would like to discuss with the Incident Management Team, please contact Chris Lines, Head of Communications with the National Public Health Service for Wales on 01443 824176.
Yours sincerely,
Grace Lewis Parry
Chief Executive
6b Letter regarding conclusion of the Lookback
Sent to all patients originally advised of the need for testing
Dear
Testing for a blood borne virus due to your possible exposure in a health care setting
I am writing to inform you of the conclusions of our work following diagnosis of hepatitis C in a health care worker in Gwynedd.
From our investigations into a very large number of patients, we have found no evidence of anyone being infected with hepatitis C, hepatitis B or HIV by the health care worker.
Hepatitis C
The health care worker was diagnosed with hepatitis C. That’s what prompted our offer of screening to those patients for whom we had written records.
We tested the health care worker’s patients in case blood to blood contact with the health care worker led to the infection of a patient. Of the 2,665 patients tested, eleven are, or have been, infected with hepatitis C. This is what we would expect in a population of this size.
Where we were able to further test the blood of the eleven, we can show that all had a different type of hepatitis C to that of the health care worker. With the others, detailed interviewing showed that they had been exposed to risks well known to getting hepatitis C. For example, intravenous drug users or people who had a blood transfusion before 1991 (when blood products were first tested for hepatitis C) are known to be at greater risk than others.
There is therefore no evidence of anyone being infected with hepatitis C by the health care worker.
For the same reasons, there is also no evidence of any patient infecting another patient during treatment by the health care worker.
Hepatitis B
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 48 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
The health care worker did not have hepatitis B. However, we tested the blood of the healthcare worker’s patients in case it had been passed from patient to patient in the health care setting – a very unlikely event.
Of the 2,665 people tested, not one was found to have hepatitis B. Twenty were found to have had the infection at some time in the past. This is the sort of number we would expect in a population of this size.
Detailed interviewing of 18 of the 20 showed that they had been exposed to risks well known to getting hepatitis B. For example, intravenous drug users or people who had a blood transfusion before 1987 (when blood products were first tested for hepatitis B) are known to be at greater risk than others.
Detailed questioning about the health care treatment received by these people showed that it is extremely unlikely that the infection could have been caught in this way.
I therefore conclude that there is no evidence of a single patient being infected of hepatitis B by blood to blood contact with another of the health care worker’s patients.
HIV
The health care worker did not have HIV. However, for the same reasons as we tested for hepatitis B, we also tested the blood of the health care worker’s patients in case it had been passed from patient to patient in the healthcare setting – an even more unlikely event.
Of the 2,665 people tested, not one was found to have, or have had, HIV.
I am therefore certain that not one of the patients we tested for HIV could have passed it on to another of the health care worker’s patients.
Conclusions
We have shared our findings with UK experts – the United Kingdom Advisory Panel for blood borne viruses. They share our view that there is no evidence to justify any further action.
The evidence shows that patients of the health care worker are at no greater risk than the wider population. As such, we do not need to take any further action.
I hope you find this reassuring.
This whole process has taken many months. I hope you understand that it was very important that we respected the rights of all the patients involved, that we completed our work in the most thorough way possible and that we acted on the advice of experts.
I am writing to all patients who we contacted or who have self-identified. We are also briefing the media so I expect there to be media coverage on Wednesday 21 March.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 49 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Yours sincerely
Dr Sandra Payne
Director of Public Health
P.S. For a copy of the Incident Management Team’s report into the Look Back and further information on the Look Back and the infections please visit the National Public Health Service for Wales web site – www.nphs.wales.nhs.uk
6c Letter regarding conclusion of the Lookback
Sent to all patients who self identified
Dear
Testing for a blood borne virus due to your possible exposure in a health care setting
I am writing again following your concern about getting hepatitis C from a health care worker in Gwynedd.
From our investigations into a very large number of patients, we have found no evidence of anyone being infected with hepatitis C, hepatitis B or HIV by the health care worker.
Hepatitis C
The health care worker was diagnosed with hepatitis C. That’s what prompted our offer of screening to those patients for whom we had written records.
We tested the health care worker’s patients in case blood to blood contact with the health care worker led to the infection of a patient. Of the 2,665 patients tested, eleven are, or have been, infected with hepatitis C. This is what we would expect in a population of this size.
Where we were able to further test the blood of the eleven, we can show that all had a different type of hepatitis C to that of the healthcare worker. With the others, detailed interviewing showed that they had been exposed to risks well known to getting hepatitis C. For example, intravenous drug users or people who had a blood transfusion before 1991 (when blood products were first tested for hepatitis C) are known to be at greater risk than others.
There is therefore no evidence of anyone being infected with hepatitis C by the health care worker.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 50 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
For the same reasons, there is also no evidence of any patient infecting another patient during treatment by the health care worker.
Hepatitis B
The health care worker did not have hepatitis B. However, we tested the blood of the health care worker’s patients in case it had been passed from patient to patient in the health care setting – a very unlikely event.
Of the 2,665 people tested, not one was found to have hepatitis B. Twenty were found to have had the infection at some time in the past. This is the sort of number we would expect in a population of this size.
Detailed interviewing of 18 of the 20 showed that they had been exposed to risks well known to getting hepatitis B. For example, intravenous drug users or people who had a blood transfusion before 1987 (when blood products were first tested for hepatitis B) are known to be at greater risk than others.
Detailed questioning about the health care treatment received by these people showed that it is extremely unlikely that the infection could have been caught in this way.
I therefore conclude that there is no evidence of a single patient being infected of hepatitis B by blood to blood contact with another of the health care worker’s patients.
HIV
The healthcare worker did not have HIV. However, for the same reasons as we tested for hepatitis B, we also tested the blood of the healthcare worker’s patients in case it had been passed from patient to patient in the health care setting – an even more unlikely event.
Of the 2,665 people tested, not one was found to have, or have had, HIV.
I am therefore certain that not one of the patients we tested for HIV could have passed it on to another of the health care worker’s patients.
Conclusions
We have shared our findings with UK experts – the United Kingdom Advisory Panel for blood borne viruses. They share our view that there is no evidence to justify any further action.
The evidence shows that patients of the health care worker are at no greater risk than the wider population. As such, we do not need to offer you a blood test.
I hope you find this reassuring.
Thank you for your patience. This whole process has taken many months. I hope you understand that it was very important that we respected the rights of all the patients
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 51 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report involved, that we completed our work in the most thorough way possible and that we acted on the advice of experts.
Yours sincerely
Dr Sandra Payne
Director of Public Health
P.S. You can find further information about hepatitis C, hepatitis B and HIV - and about the work of the team looking back for evidence of infection – on the web site of the National Public Health Service for Wales – www.nphs.wales.nhs.uk
6d Letter regarding conclusion of the Lookback
An example is given below of the core text used in letters which were sent to
1. CHCs, AMs, MPs, Party health spokespeople, Gwynedd County Councillors, Gwynedd community councillors
2. Dentists, GPs / Practice Managers, community pharmacists
3. North West Wales NHS Trust (for cascade to front line staff)
4. CMO, Director DHSS, CHC chief officers, neighbouring Trust and LHB chief executives, HIW chief executive, Local Dental Committee, Local Medical Committee
Dear
Testing for a blood borne virus due to possible exposure in a health care setting
I am writing to inform you of the conclusions of our work following diagnosis of hepatitis C in a health care worker in Gwynedd.
From our investigations into a very large number of patients, we have found no evidence of anyone being infected with hepatitis C, hepatitis B or HIV by the health care worker.
Hepatitis C
The health care worker was diagnosed with hepatitis C. That’s what prompted our offer of screening to those patients for whom we had written records.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 52 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
We tested the health care worker’s patients in case blood to blood contact with the health care worker led to the infection of a patient. Of the 2,665 patients tested, eleven are, or have been, infected with hepatitis C. This is what we would expect in a population of this size.
Where we were able to further test the blood of the eleven, we can show that all had a different type of hepatitis C to that of the health care worker. With the others, detailed interviewing showed that they had been exposed to risks well known to getting hepatitis C. For example, intravenous drug users or people who had a blood transfusion before 1991 (when blood products were first tested for hepatitis C) are known to be at greater risk than others.
There is therefore no evidence of anyone being infected with hepatitis C by the health care worker.
For the same reasons, there is also no evidence of any patient infecting another patient during treatment by the health care worker.
Hepatitis B
The health care worker did not have hepatitis B. However, we tested the blood of the healthcare worker’s patients in case it had been passed from patient to patient in the health care setting – a very unlikely event.
Of the 2,665 people tested, not one was found to have hepatitis B. Twenty were found to have had the infection at some time in the past. This is the sort of number we would expect in a population of this size.
Detailed interviewing of 18 of the 20 showed that they had been exposed to risks well known to getting hepatitis B. For example, intravenous drug users or people who had a blood transfusion before 1987 (when blood products were first tested for hepatitis B) are known to be at greater risk than others.
Detailed questioning about the health care treatment received by these people showed that it is extremely unlikely that the infection could have been caught in this way.
I therefore conclude that there is no evidence of a single patient being infected of hepatitis B by blood to blood contact with another of the health care worker’s patients.
HIV
The health care worker did not have HIV. However, for the same reasons as we tested for hepatitis B, we also tested the blood of the health care worker’s patients in case it had been passed from patient to patient in the healthcare setting – an even more unlikely event.
Of the 2,665 people tested, not one was found to have, or have had, HIV.
I am therefore certain that not one of the patients we tested for HIV could have passed it on to another of the health care worker’s patients. Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 53 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Conclusions
We have shared our findings with UK experts – the United Kingdom Advisory Panel for blood borne viruses. They share our view that there is no evidence to justify any further action.
The evidence shows that patients of the health care worker are at no greater risk than the wider population. As such, we do not need to take any further action.
I hope you find this reassuring.
This whole process has taken many months. I hope you understand that it was very important that we respected the rights of all the patients involved, that we completed our work in the most thorough way possible and that we acted on the advice of experts.
I am writing to all patients who we contacted or who have self-identified. We are also briefing the media so I expect there to be media coverage on Wednesday 21 March.
Yours sincerely
Dr Sandra Payne
Director of Public Health
P.S. You can find further information about the Look Back and its conclusions on the web site of the National Public Health Service for Wales – www.nphs.wales.nhs.uk
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 54 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 7 Follow-up of positive results
Communications with GPs and patients
Positive or equivocal results were telephoned by the microbiologist at NWWT to the patient’s GP, at the time the test report was issued by the Bangor laboratory, and the significance of the result explained. This was followed up by a letter to the GP which confirmed the results, explained the significance of these results for the individual, how the patient would be managed as part of the case-control study, advice on clinical management and onward referral, and also outlined the next steps to take.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 55 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Example of letter to GP:
Preswylfa Preswylfa Ffordd Hendy Hendy Road YR WYDDGRUG MOLD Sir Y Fflint Flintshire CH7 1PZ CH7 1PZ Ffon: 01352 803234 Tel: 01352 803234 Ffacs: 01352 700043 Fax: 01352 700043
26 June 2006
Dr XXXX address
Dear Dr XXXX
Re: Patient name, dob, NHS number, lookback ID number
The results of blood tests for your patient as part of the Gwynedd healthcare worker look back investigation are as follows:
Hepatitis B surface antigen negative
Hepatitis C antibody positive
HIV negative
This result indicates infection with hepatitis C at some time. It is not possible to say if there is evidence of current infection from the sample tested.
The implications of this result are that:
1. Further sampling, as described below, is required to determine if the patient is still infected with hepatitis C. If there is no current infection then the infection has been cleared. If there is current infection, it may be passed on to others and the patient should be advised about lifestyle and occupational implications.
2. A repeat sample of clotted blood is required to confirm the serology, and a sample of whole blood (EDTA sample) is required to determine if there is evidence of current infection.
3. It is not possible to say at this stage if the infection may have been contracted either from the health care worker, or as a result of the health care worker’s practice.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 56 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Please would you arrange to:
1. Inform your patient as soon as possible of these results and discuss the result with them. Please bear in mind that patients will be telephoning NHS Direct three weeks after the blood sample was taken in the expectation of receiving a negative result.
2. Refer the patient to Dr YYYY in Gastroenterology in Ysbyty Gwynedd, to discuss the test results and to enable the further sampling described above. The referral must state that this is a look back patient. The hospital Trust is arranging appointments specifically for the look back patients.
3. Inform your patient that they will be contacted by a member of the North Wales Health Protection Team. Please obtain the patient’s preferred method of contact, e.g. telephone, letter (see what we will do, below). Once you have done this, please inform the Health Protection Team on 01352 803 234 (9am – 5pm).
What the NPHS and Gwynedd Local Health Board will do:
1. If follow-up tests indicate the patient is still infected with hepatitis C, we will inform you of the result, and Dr YYYY will then see the patient again to discuss the test results and treatment options.
2. A member of the North Wales Heath Protection Team will contact your patient (see above) to discuss any issues. They will arrange a convenient time to interview her/him to ask about previous risk factors such as lifestyle and previous medical history, and to fill in a questionnaire. This will be analysed as part of a case-control study.
3. We will inform you of the results of the look back investigation when they are available.
I stress that evidence of infection of patients as a result of treatment by the health care worker may not be demonstrated conclusively by the investigation.
Thank you for your help and co-operation in this investigation.
If you have any questions about the arrangements, please contact the North Wales Health Protection Team on 01352 803 234.
Yours sincerely,
Dr Chris Whiteside Consultant in Communicable Disease Control
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 57 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 8 RNA Sequencing
There are 11 major variants of the genetic structure of the Hepatitis C virus. These variants can be subdivided into smaller groups, and these groups are called genotypes. Genotyping is the process by which a Hepatitis C virus infection is identified as belonging to one of these specific groups. Variations in genetic structure exist within any given genotype. These variations can be identified by detecting differences in the order in which the molecules composing the genes are arranged. Any such differences determine whether infecting viruses are the same, and if not the same, how closely related they are. The process of identifying the order in which these molecules are arranged within a gene is called sequencing.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 58 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 9 Case control Study
Communication with GPs and patients
All patients who tested positive for one of the blood borne viruses were asked to participate in the case control study. Letters were sent to GPs of positive or equivocal patients in North Wales the day that blood results were available. For patients out of North Wales patients, the local Health Protection Teams contacted GPs. The letter (see above example) asked that the GP inform patients of the test results, the nature of the case control study, and to ask the patients to agree to be contacted by a member of the North Wales Health Protection Team (either by letter or telephone) to arrange for an interview (appx letter GP). This was offered either face to face or by telephone in the patient’s choice of English or Welsh language. Those patients with equivocal results who subsequently tested negative were not approached further. It was emphasised in the letter that the patients be informed as soon as possible of positive results, as the patients would be telephoning NHSD in anticipation of a negative result two weeks after their blood was tested.
Where GPs had not responded to the initial request regarding patient interview or patient had not contacted the HPT, the GP was telephoned to remind them about contacting their patients. Where necessary GPs were also reminded to arrange clinical follow up and blood tests for their patients.
If no answer had been received by the end of July 2006, a letter was sent directly to the patient. A reminder letter was then mailed to those still outstanding after a further five working days. As a result twenty-five ‘positive’ patients were contacted and interviewed by the HPT.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 59 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Case Letter
Preswylfa Preswylfa Ffordd Hendy Hendy Road YR WYDDGRUG MOLD Sir Y Fflint Flintshire CH7 1PZ CH7 1PZ Ffon: 01352 803234 Tel: 01352 803234 Ffacs: 01352 700043 Fax: 01352 700043
Date ID ref: ####
Pt name and address
Dear
As part of the Gwynedd healthcare worker look back investigation, you have recently been informed by your doctor of your blood test results and the need for a member of the North Wales health protection team to complete a confidential interview with you. The aim of the interview is to try and identify where your infection may have come from.
To arrange this interview would you please call the North Wales Health Protection Team on 01352 803234 or 803255 (9am – 5pm). Interviews can be conducted in Welsh or English, face to face or over the telephone as preferred.
This is an important part of the investigation and I would like to thank you for your help and continued co-operation.
Yours sincerely,
Dr Chris Whiteside
Consultant in Communicable Disease Control
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 60 of 78 Management Team National Public Health Service for Wales
Preswylfa, Hendy Road, Mold. CH7 1PZ Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Case Letter 2
Preswylfa Preswylfa Ffordd Hendy Hendy Road YR WYDDGRUG MOLD Sir Y Fflint Flintshire CH7 1PZ CH7 1PZ Ffon: 01352 803234 Tel: 01352 803234 Ffacs: 01352 700043 Fax: 01352 700043
02 August 2006 ID Ref:####
Pt name and address
Dear
Your blood test results from the Gwynedd healthcare worker look back investigation are now available from your doctor. You may have already been contacted by your doctor, but if you have not received, or are uncertain of your results, please contact your surgery. As part of the investigation, a member of the North Wales Health Protection Team needs to complete a confidential interview with you, the aim of which is to try to identify where infections may have come from.
To arrange this interview would you please call the North Wales Health Protection Team on 01352 803234 or 803255 (9am – 5pm) in the next 5 working days. If you have not managed to arrange the interview by this time, we will need to contact you directly to discuss this further. Interviews can be conducted in Welsh or English, face to face or over the telephone, as preferred.
This is an important part of the investigation and I would like to thank you for your help and continued co-operation.
Yours sincerely,
Dr Chris Whiteside Consultant in Communicable Disease Control
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 61 of 78 Management Team National Public Health Service for Wales
Preswylfa, Hendy Road, Mold. CH7 1PZ Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Case and control patient interviews for case-control study
Four controls per case (120 controls) were selected randomly and letters (see Control letter) sent to these individuals at the end of July 2006. If no contact was received within ten days, a further letter was sent.
Members of the North Wales HPT conducted telephone interviews with twenty-five patients with positive virology – eight of eleven patients with hepatitis C, and eighteen of twenty with past infection with hepatitis B. One patient had been infected with both hepatitis B and C. Sixty-seven controls agreed to be interviewed.
Five interviewers were used, as this was considered a minimum to allow flexibility in timing for patients, as some wanted to be contacted out of office hours, but allowed the interviewers to continue their normal work schedule. One of the interviewers led a training session for the other four, who then followed a written proforma to ensure consistency and minimise interviewer bias as far as possible.
Interviewees were asked to sign a form giving their consent to allow an investigator to look at past clinical records pertaining to treatment by the HEALTH CARE WORKER if needed (see Consent form).
Completed questionnaires were then analysed as part of the case-control study at the Communicable Disease Surveillance Centre (CDSC) Cardiff.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 62 of 78 Management Team National Public Health Service for Wales
Preswylfa, Hendy Road, Mold. CH7 1PZ Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
First letter to controls
Preswylfa Preswylfa Ffordd Hendy Hendy Road YR WYDDGRUG MOLD Sir Y Fflint Flintshire CH7 1PZ CH7 1PZ Ffon: 01352 803234 Tel: 01352 803234 Ffacs: 01352 700043 Fax: 01352 700043
27 July 2006 ID Ref:####
Name / address
Dear
As part of the Gwynedd healthcare worker look back investigation, the North Wales Health Protection Team needs to complete a confidential interview to allow comparisons to be made between people whose results were normal and those with infection. You have been randomly selected from all the people who were tested and had clear results. If you have not received, or are uncertain of your results, please contact NHS Direct on 0845 4647, before responding to this letter.
This is an important part of the investigation and interviews will only take 15-20 minutes. To arrange the interview, would you please call the North Wales Health Protection Team on 01352 803234 or 803255 (9am – 5pm) in the next 5 working days. If you have not managed to arrange the interview by this time, we will contact you again. Interviews can be conducted at your convenience in Welsh or English, face to face or over the telephone, as preferred.
I would like to thank you for your help and continued co-operation.
Yours sincerely,
Dr Chris Whiteside
Consultant in Communicable Disease Control Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 63 of 78 Management Team National Public Health Service for Wales
Preswylfa, Hendy Road, Mold. CH7 1PZ Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Second letter to controls
Preswylfa Preswylfa Ffordd Hendy Hendy Road YR WYDDGRUG MOLD Sir Y Fflint Flintshire CH7 1PZ CH7 1PZ Ffon: 01352 803234 Tel: 01352 803234 Ffacs: 01352 700043 Fax: 01352 700043
07 August 2006 ID Ref:####
Name / address
Dear
I recently wrote to you about the need to contact you as part of the Gwynedd healthcare worker look back investigation. A member of the North Wales Health Protection Team needs to complete a confidential interview with you to allow comparisons to be made between people whose results were normal and those with infection. You have been randomly selected from all the people who were tested and had clear results.
This is an important part of the investigation and interviews will only take 5-15 minutes. To arrange the interview, would you please call the North Wales Health Protection Team on 01352 803234 or 803255 (9am – 5pm) in the next 5 working days. Interviews can be conducted at your convenience in Welsh or English, face to face or over the telephone, as preferred. Your help in this investigation is appreciated, and I would like to thank you for your continued co-operation. Yours sincerely,
Dr Chris Whiteside
Consultant in Communicable Disease Control Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 64 of 78 Management Team National Public Health Service for Wales
Preswylfa, Hendy Road, Mold. CH7 1PZ Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Consent form Preswylfa Preswylfa Ffordd Hendy Hendy Road YR WYDDGRUG MOLD Sir Y Fflint Flintshire CH7 1PZ CH7 1PZ Ffon: 01352 803234 Tel: 01352 803234 Ffacs: 01352 700043 Fax: 01352 700043
Look back reference number □□□□
CONSENT FORM
0.1 Gwynedd health care worker look back investigation
1. I confirm that I have had explained and understand the reasons for the above investigation. I have had the opportunity to consider this information, ask questions and have had these answered satisfactorily.
2. I understand that my participation is voluntary and that I am free to withdraw at any time, without giving any reason, without my medical care or legal rights being affected.
3. I understand that relevant sections of any of my medical notes and data collected during the investigation may be looked at by responsible individuals within the National Public Health Service for Wales, from regulatory authorities or from the NHS Trust, where it is relevant to my taking part in this investigation. I give permission for these individuals to have access to my records.
4. I understand that procedures for handling, processing, storage and destruction of their data are compliant with the Data Protection Act 1998.
______
Name of Patient Date Signature
Dr Chris Whiteside ______
Consultant in Communicable Date Signature
Disease Control
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 65 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 10 Summary of Epidemiological Investigation
Investigation of Blood Borne Virus infection in individuals identified by the Gwynedd Health Care Worker patient notification exercise
1. Introduction
A healthcare worker (HCW) in Gwynedd was infected with the hepatitis C virus. A patient notification exercise was undertaken for patients treated by the HEALTH CARE WORKER. The HEALTH CARE WORKER has never been infected with the hepatitis B virus or the Human Immunodeficiency Virus (HIV) infection. However, concerns about the HEALTH CARE WORKER’s infection control practice gave rise to a risk of hepatitis B or HIV being transmitted from one patient to another. Patients were offered testing for all three Blood Borne Viruses (BBV).
2. Method
2.1 Study Design
Nested case control study.
2.2 Hypothesis
The study tested the null hypothesis that treatment by the HCW is not associated with infection with a BBV.
2.3 Cases
All individual with laboratory evidence of current or past infection with a BBV identified as a result of the Gwynedd HCW patient notification exercise.
2.4 Controls
Randomly selected individual tested as a result of the Gwynedd HCW patient notification exercise without laboratory evidence of current or past infection with a BBV.
2.5 Power
Four controls were selected per cases to give the study a statistical power of 75% at the 5% significance level to detect a 50% greater mean number of attendances at the HCW surgery in cases compared to controls.
2.6 Data Collection
Detailed information on the treatment provided by the HCW was obtained from the HCW’s records. Information on risk factors for BBV infection was obtained during telephone interviews with cases and controls.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 66 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
2.7 Analysis
Questionnaire data were collated using Epi Info 6.04 [1] and odds ratios, chi-squared tests, fishers exact test, two sided t tests , and logistic regression were calculated using STATA 8.2 [2].
3. Results
3.1 Descriptive epidemiology
As of 27th January 2006 blood samples had been tested from 2665 patients. Infection, either past or present, with the hepatitis C virus was confirmed in 11 patients and past infection with the hepatitis B virus was demonstrated in 20 patients. No patients had evidence of current infection with the hepatitis B virus or infection with HIV.
The prevalence of hepatitis C infection was 0.41% (95% CI 0.21% - 0.74%) and the prevalence of past hepatitis B infection was 0.75% (95% CI 0.46% - 1.16%).
There were no significant differences in the gender or age of cases and controls. Half (10/20) of the cases of hepatitis B, 36% (47/130) of the controls, and 36% (4/11) of the hepatitis C cases were male. The mean age of cases of hepatitis B was 60 years, controls 55 years, and cases of hepatitis C 50 years.
3.2 Analytical epidemiology
3.2.1. Hepatitis C
Table 1: Univariate analysis risk factors cases hepatitis C from review records
Treatment Cases Controls Odds 95% CI P Ratio (n=11) (n= 130)
Exposed Exposed
Yes No Yes No
>27 3 8 33 97 1.1 0.2 – 5.0 0.89 attendances
>14 2 9 30 100 0.74 0.07 – 0.71 examination 3.9
>22 procedure 3 8 30 100 1.3 0.2 – 5.6 0.75 0.77 >12 procedure 2 9 29 101 0.08 – 0.75 Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 67 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
A 4.1
>4 procedure 2 9 31 99 0.71 0.07 – 0.67 B 3.7
>2 procedure 2 9 13 117 2.0 0.19 – 0.40 C 11.2
The nature of the procedures A B, C and D are not identified to avoid identifying the occupation of the HCW.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 68 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Table 2: Number of episodes of treatment received by cases of hepatitis C
Mean number episodes
Treatment Cases Controls Difference 95% CI P
(n=11) (n=130)
Attendances 20.2 18.0 -2.1 -13, 8 0.70
Examination 10.5 9.4 -1.1 -7, 5 0.71
Any procedure 15.5 13.0 -2.5 -11, 6 0.55
Procedure A 8.9 7.3 -1.6 -7, 3 0.53
Procedure B 4.2 3.0 -1.1 -4, 1 0.37
Procedure C 1.3 1.0 -0.24 -1.2, 0.7 0.63
Procedure D 0 0.18 0.18 -0.13, 0.26 0.5
3.2.2. Hepatitis B
Table 3: Univariate analysis risk factors cases hepatitis B from review records
Treatment Cases Controls Odds 95% CI P Ratio (n=20) (n= 130)
Exposed Exposed
Yes No Yes No
>27 5 15 33 97 0.98 0.26 – 0.97 attendances 3.1
>14 5 15 30 100 1.1 0.29 – 0.85 examination 3.6
>22 procedure 5 15 30 100 1.1 0.29 – 0.85 3.6
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 69 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
0.61 >12 procedure 3 17 29 101 0.11 – 0.46 A 2.4
>4 procedure 6 14 31 99 1.4 0.40 – 0.55 B 4.2
>2 procedure 4 16 13 117 2.25 0.47 – 0.19 C 8.5
Table 4: Number of episodes of treatment received by cases of hepatitis B
Mean number episodes
Treatment Cases Controls Difference 95% CI P
(n=20) (n=130)
Attendances 19.9 18.0 -1.8 -10, 7 0.68
Examination 10.8 9.4 -1.4 -6, 3 0.57
Any procedure 14.6 13.0 -1.6 -8, 5 0.63
Procedure A 7 7.3 0.3 -4, 4 0.90
Procedure B 4.3 3.0 -1.3 -3, 1 0.24
Procedure C 1.7 1.0 -0.7 -1.5, 0.2 0.13
Procedure D 0 0.18 0.18 -0.5, 0.4 0.13
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 70 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
3.3 Virological investigations cases hepatitis C
Case Genotype Sequencing Alternative Risk Factors*
1 1 Different from cases 3, 5, and 11
2 Not available Declined testing Yes
3 1a Different from cases 1, 5 and 11
4 Mixed Sample unsuitable Yes
5 1a Different from cases 1, 3, and 11
6 2 No other genotype 2
7 Not available Not viraemic Yes
8 3a Different from HCW and case 9
9 3a Different from HCW and case 8
10 Not available Not viraemic Yes
11 1a Different from cases 1, 3 and 5.
*The presence of alternative risk factors are only identified when virus was not available for sequencing.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 71 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
4. Discussion
4.1 Transmission Hepatitis C from the HCW to patients
The observed prevalence of hepatitis C virus infection of 0.41% (95% CI 0.21% - 0.74%) is similar to the estimated prevalence of hepatitis C virus in England of 0.5% [3]. Eight of the 11 cases of hepatitis C virus infection agreed to be interviewed. Seven of these 8 cases had other risk factors for hepatitis C infection.
Analytical epidemiology did not demonstrate any statistically significant association between treatment and infection with the hepatitis C virus. However, the small number of cases limits the power of this part of the study to detect a difference if one existed.
The HCW was infected with a genotype 3a virus. Sequencing of virus isolated from the two patients with genotype 3a infection demonstrated that the viruses were not related to the HCW. The four patients from whom virus was unobtainable all had alternative explanations for their hepatitis C virus infection.
There is no evidence which demonstrates transmission of the hepatitis C virus from the HCW to a patient. The evidence available from patients who presented from testing suggests that this is extremely unlikely to have occurred in this group of patients.
It is difficult to absolutely prove a negative. This would require all patients to present for testing and for virus to be recovered from all patients with evidence of hepatitis C virus infection. Under half of the patients who were known to have been treated by the HCW were tested. The findings in these patients suggest that the risk of transmission from the HCW to patients is low.
4.2 Transmission of BBV from patient to patient
4.2.1 HIV
No patients tested positive for HIV infection and thus patient to patient transmission of HIV did not occur in the patients who were tested.
4.2.2 Hepatitis C
As discussed in section 4.1 the observed prevalence of hepatitis C virus infection was not elevated and the case-control study did not show any association between infection and the amount of treatment.
Sequencing of virus isolated from the two patients with genotype 3a infection demonstrated that the viruses were not related to each other. Sequencing of virus isolated from the four patients with genotype 1 or 1a infection demonstrated that the viruses were not related to each other. The four patients from whom virus was
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 72 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report unobtainable all had risk factors for hepatitis C virus infection that were a more likely source than patient to patient treatment during treatment.
There is no evidence which demonstrates patient to patient transmission of the hepatitis C virus during treatment by the HCW. The available evidence suggests that patient to patient transmission arising from any deficiency in infection control practice is very unlikely to have occurred in the patients who were tested.
4.2.3 Hepatitis B
Data with which to compare the observed prevalence of past hepatitis B virus infection of 0.75% (95% CI 0.46% - 1.16%) is limited. A 1998 population based study in the Republic of Ireland found anti-HBc in 0.29% (5/1714) of specimens tested [4]. A 1996 study of residual diagnostic sera in England and Wales found anti-HBc in 2.5% (75/3039) of specimens tested from outside of London [5]. However, the prevalence in these selected samples in different areas was highly dependent on the proportion of the population born in Africa and Asia. In Gwynedd only 1.6% of the population was born outside of the European Union and as a result the predicted prevalence from these data would be much lower than 2.5%. A study of blood donors in the South West of England in1979 reported a prevalence of anti-HBc of 0.7% in new donors and 0.4% in established donors [6]. The prevalence in West Yorkshire firemen in 1988 was reported as 0.6% (1/173) [7] and in Lancashire police officers 2.8% (8/284) [8]. The observed prevalence, 0.76%, of anti-HBc in this investigation is probably at a level that might reasonable be expected.
Interviews have been completed with 18 of the 20 cases of hepatitis B virus infection.
Seven of these 18 cases had other high risk exposures for hepatitis B infection and the remaining 11 had exposure that could have accounted for hepatitis B infection.
Analytical epidemiology did not demonstrate any statistically significant association between treatment and infection with the hepatitis B virus. No patients where found to have current infection with the hepatitis B virus and thus to have presented a risk to other patients for a prolonged period of time. The prevalence of past hepatitis B infection was not elevated.
There is no evidence which demonstrates patient to patient transmission of the hepatitis B virus during treatment by the HCW. The available evidence suggests that risk of patient to patient transmission of the hepatitis B virus arising from deficiency in infection control practice is low.
4.2.4 Conclusion transmission of BBV from patient to patient
The initial risk assessment conducted by the NPHS concluded that the risk of patient to patient transmission of a BBV infection was probably very small but not zero. The assessment was reliant on there being a low prevalence of BBV infections in the relevant community rather than on the safety of the infection control procedures in peration.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 73 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Testing demonstrated that the assumption underpinning the initial risk assessment was correct. No cases of HIV or current hepatitis B infection were detected. Patients with evidence of past hepatitis B infection will have been infectious for relatively short periods of time in the past. It is not possible to date the onset of hepatitis B infection and thus determine if individuals were infectious at the time they received treatment.
The only known stress on the infection control procedures during treatment provided by the HCW were patients with hepatitis C infection. In general terms the risk of transmission from patients with circulating virus in a healthcare setting is intermediate for hepatitis C between the higher risk for hepatitis B and lower risk for HIV. The patients with hepatitis C virus identified as part of this patient notification were unlikely to have acquired the infection as a result of treatment.
It is difficult to absolutely prove a negative. This would require all patients to present for testing and for virus to be recovered from all patients with evidence of BBV virus infection. Under half of the patients who were known to have been treated by the HCW were tested. Investigation of these patients suggests that the risk of patient to patient transmission is low.
5. Conclusion
5.1 Extension of patient notification to patients who were not identified from HCW records and have not self identified
The original advice from the UKAP was to notify patients who could be identified from the HCW records. In the absence of any documented transmission and confirmation of the original risk assessment there is no indication to extent the patient notification exercise. It would be disproportionate to name the HCW in the public domain to enable patients to self identify.
5.2 Extension of patient notification to patients who have self identified
The original decision taken by the IMT was not to offer testing to patients who self identify. The situation has not changed materially since this decision was taken. In the absence of any documented transmission and confirmation of the original risk assessment there is no new indication to offer testing to patients who have self identified.
6. Recommendation
The IMT considers this report to determine its preferred option for concluding this patient notification exercises. The IMTs decision and supporting rationale is communicated to UKAP for advice to confirm that the decision taken by the IMT is reasonable.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 74 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
References
[1] Epidemiology Program Office. Epi Info Version 6.04d. Atlanta:Centers for Disease Control and Prevention, 2001.
[2] StataCorp. Stata Statistical Software: Release 8.2. Texas: Stata Corporation, 2004.
[3] Health Protection Agency. Hepatitis C in England. The First Health Protection Agency Annual Report 2005. London: HPA, 2005.
[4] O’Connell T et al. Prevalence of heapatitis B anti-core antibody in the Republic of Ireland. Epidemiology & Infection 2000;125:701-704.
[5] Gay NJ et al. The prevalence of hepatitis B infection in adults in England and Wales. Epidemiology & Infection 1999;122:133-138.
[6] Archer AC, Cohen BJ, Mortimer PP. The value of screening blood donors for antibody to hepatitis B core antigen. Journal of Clinical Pathology 1983;36:924-928.
[7] Crosse BA, Teale C, Lees EM. Hepatitis B markers in West Yorkshire firemen. Epidemiology & Infection 1999;1203:383-385.
[8] Morgan-Capner P, Hudson P. Hepatitis B markers in Lancashire police officers. Epidemiology & Infection 1999;100:145-151.
Notes
As the patient notification exercise was still on going when the case control study was started a slight excess of the planed 4 controls per case were selected for interview (120 controls) and review of notes (these 120 controls + 10 further controls) to ensure that sufficient controls are available when the process wais completed.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 75 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
Appendix 11 Timetable of events
2005
3rd October Gwynedd Local Health Board and the National Public Health Service for Wales (NPHS) were notified of the healthcare worker being diagnosed with Hepatitis C.
3rd October The healthcare worker stopped working.
5th October The first Incident Management Team meeting was held. At this meeting, the need for further advice was discussed.
21st October Following further consideration, the Incident Management Team wrote to the United Kingdom Advisory Panel (UKAP) for Blood Borne Viruses formally seeking advice on action to take.
14th December UKAP responded to the Incident Management Team’s letter.
21st December The UKAP letter was received. It advised that the Incident Management Team should conduct a Look Back of the healthcare worker’s patients.
29th December A meeting of the Incident Management Team was held and formally agreed to conduct the Look Back
2006
11th January The Incident Management Team formally wrote to the healthcare worker requesting all patient notes.
18th January Incident Management Team meeting
7th February Incident Management Team meeting
7th March Incident Management Team meeting
8th March After ongoing discussions a second formal request for the patient notes was sent.
22nd March The first set of patient notes was received by the Incident Management Team.
Incident Management Team meeting
6th April The final set of patient notes was received from the healthcare worker.
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 76 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
7th April Incident Management Team meeting
28th April Data collection phase completed.
2nd May Incident Management Team meeting
10th May BBC Wales contacted the LHB and NPHS with information on the Look Back.
12th May Despite representations about the public concern that would be generated, BBC Wales broadcasts news of the Look Back.
12th May Incident Management Team meeting
13th May Incident Management Team meeting
15th May Incident Management Team meeting
16th May Incident Management Team meeting
19th May Incident Management Team meeting
24th May Letter received from UKAP advising that the Look Back should cover Hepatitis B and HIV as well as Hepatitis C.
Incident Management Team meeting
26th May Incident Management Team meeting
30th May Letters sent to patients notifying them of the risk and offering advice, support and a blood test.
30th May Incident Management Team meeting
1st June Incident Management Team meeting – a.m.
Incident Management Team meeting – p.m.
5th June First of the clinics held to take blood tests
8th June Incident Management Team meeting
15th June Incident Management Team meeting
21st June Incident Management Team meeting
4th July Incident Management Team meeting
17th July Last of the clinics to take blood tests held
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 77 of 78 Management Team Look Back Incident Management Team Draft Hepatitis C Look Back IMT Report
20th July Incident Management Team meeting
21st August Incident Management Team meeting
13th September Incident Management Team meeting
4th October Incident Management Team meeting
Version: 13 Date: 13/3/07 Status: Approved by the Incident Author: Jo Charles, Rob Atenstaedt. Page: 78 of 78 Management Team