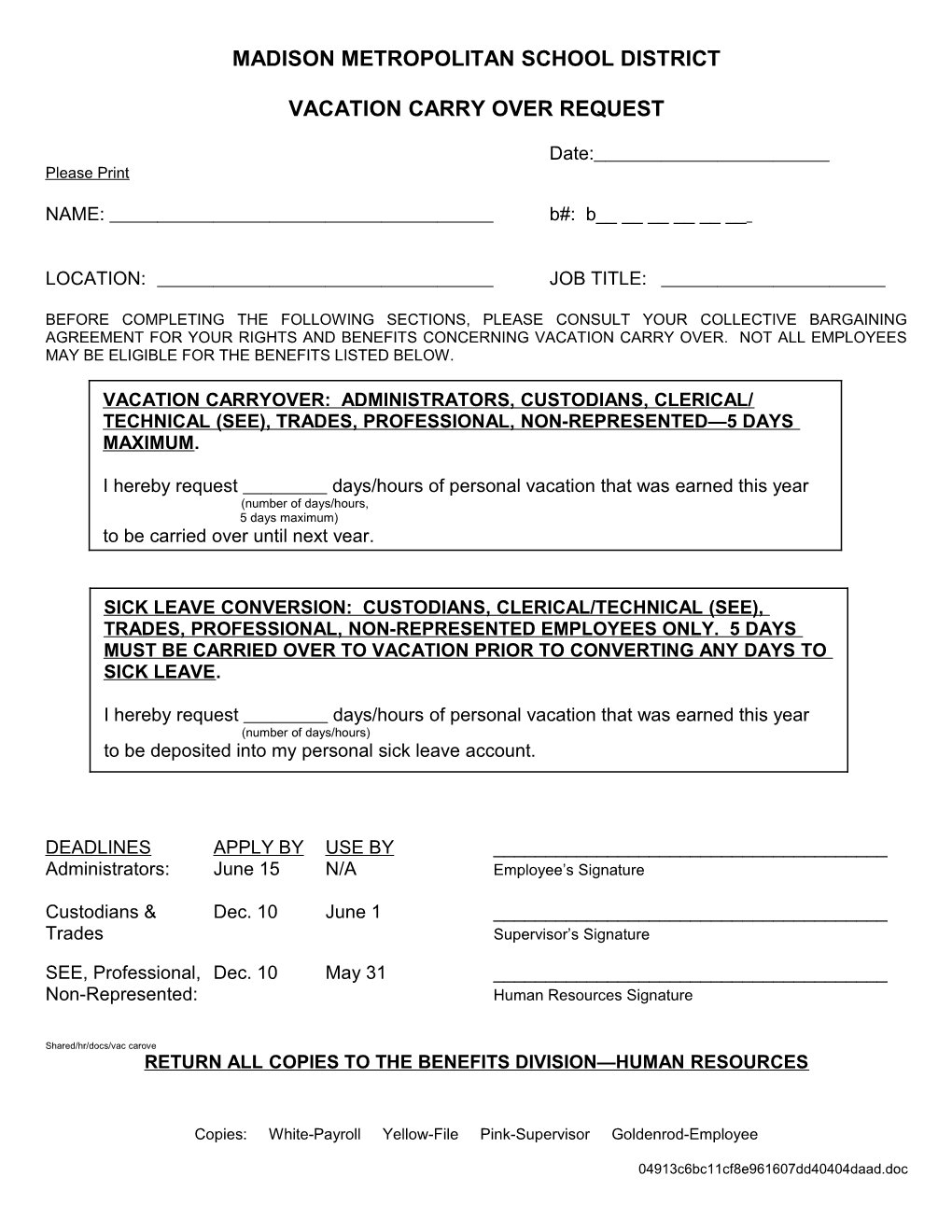
MADISON METROPOLITAN SCHOOL DISTRICT
VACATION CARRY OVER REQUEST
Date: Please Print
NAME: b#: b______
LOCATION: JOB TITLE:
BEFORE COMPLETING THE FOLLOWING SECTIONS, PLEASE CONSULT YOUR COLLECTIVE BARGAINING AGREEMENT FOR YOUR RIGHTS AND BENEFITS CONCERNING VACATION CARRY OVER. NOT ALL EMPLOYEES MAY BE ELIGIBLE FOR THE BENEFITS LISTED BELOW.
VACATION CARRYOVER: ADMINISTRATORS, CUSTODIANS, CLERICAL/ TECHNICAL (SEE), TRADES, PROFESSIONAL, NON-REPRESENTED—5 DAYS MAXIMUM.
I hereby request days/hours of personal vacation that was earned this year (number of days/hours, 5 days maximum) to be carried over until next year.
SICK LEAVE CONVERSION: CUSTODIANS, CLERICAL/TECHNICAL (SEE), TRADES, PROFESSIONAL, NON-REPRESENTED EMPLOYEES ONLY. 5 DAYS MUST BE CARRIED OVER TO VACATION PRIOR TO CONVERTING ANY DAYS TO SICK LEAVE.
I hereby request days/hours of personal vacation that was earned this year (number of days/hours) to be deposited into my personal sick leave account.
DEADLINES APPLY BY USE BY ______Administrators: June 15 N/A Employee’s Signature
Custodians & Dec. 10 June 1 ______Trades Supervisor’s Signature
SEE, Professional, Dec. 10 May 31 ______Non-Represented: Human Resources Signature
Shared/hr/docs/vac carove RETURN ALL COPIES TO THE BENEFITS DIVISION—HUMAN RESOURCES
Copies: White-Payroll Yellow-File Pink-Supervisor Goldenrod-Employee
04913c6bc11cf8e961607dd40404daad.doc