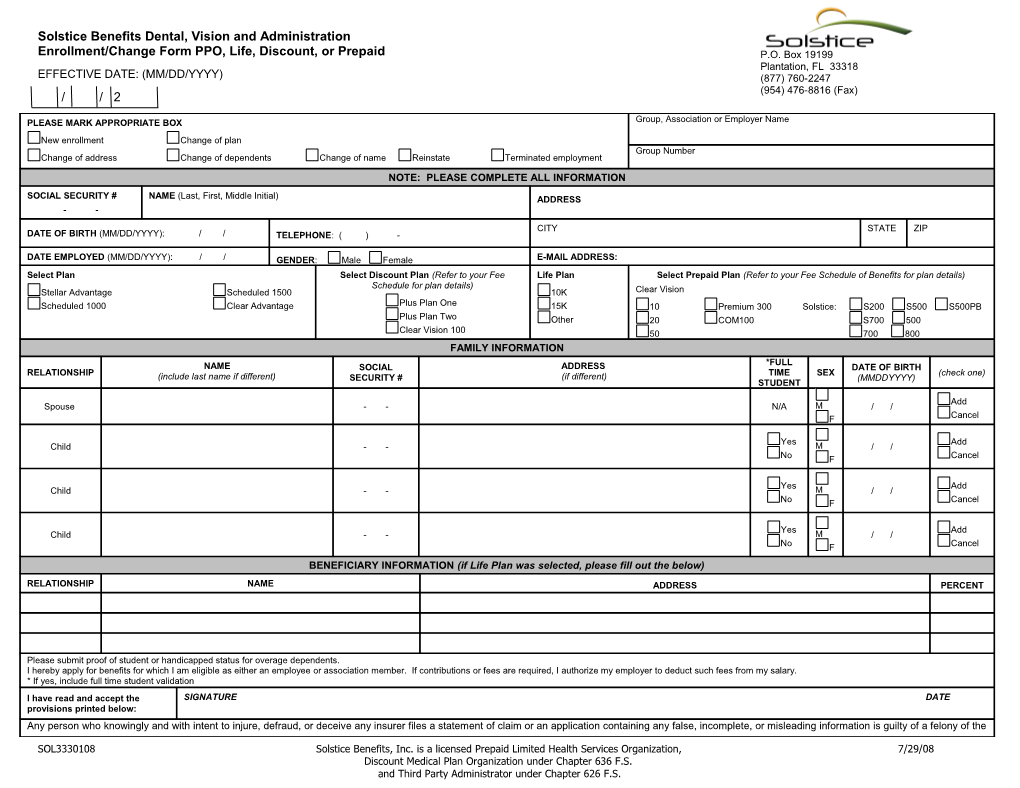
Solstice Benefits Dental, Vision and Administration Enrollment/Change Form PPO, Life, Discount, or Prepaid P.O. Box 19199 Plantation, FL 33318 EFFECTIVE DATE: (MM/DD/YYYY) (877) 760-2247 (954) 476-8816 (Fax) / / 2
PLEASE MARK APPROPRIATE BOX Group, Association or Employer Name
New enrollment Change of plan Group Number Change of address Change of dependents Change of name Reinstate Terminated employment NOTE: PLEASE COMPLETE ALL INFORMATION
SOCIAL SECURITY # NAME (Last, First, Middle Initial) ADDRESS - -
CITY STATE ZIP DATE OF BIRTH (MM/DD/YYYY): / / TELEPHONE: ( ) -
DATE EMPLOYED (MM/DD/YYYY): / / GENDER: Male Female E-MAIL ADDRESS: Select Plan Select Discount Plan (Refer to your Fee Life Plan Select Prepaid Plan (Refer to your Fee Schedule of Benefits for plan details) Schedule for plan details) Stellar Advantage Scheduled 1500 10K Clear Vision Scheduled 1000 Clear Advantage Plus Plan One 15K 10 Premium 300 Solstice: S200 S500 S500PB Plus Plan Two Other 20 COM100 S700 500 Clear Vision 100 50 700 800 FAMILY INFORMATION *FULL NAME SOCIAL ADDRESS DATE OF BIRTH RELATIONSHIP TIME SEX (check one) (include last name if different) SECURITY # (if different) (MMDDYYYY) STUDENT
Add Spouse - - N/A M / / F Cancel
Yes Add Child - - M / / No F Cancel
Yes Add Child - - M / / No F Cancel
Yes Add Child - - M / / No F Cancel BENEFICIARY INFORMATION (if Life Plan was selected, please fill out the below)
RELATIONSHIP NAME ADDRESS PERCENT
Please submit proof of student or handicapped status for overage dependents. I hereby apply for benefits for which I am eligible as either an employee or association member. If contributions or fees are required, I authorize my employer to deduct such fees from my salary. * If yes, include full time student validation I have read and accept the SIGNATURE DATE provisions printed below: Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the
SOL3330108 Solstice Benefits, Inc. is a licensed Prepaid Limited Health Services Organization, 7/29/08 Discount Medical Plan Organization under Chapter 636 F.S. and Third Party Administrator under Chapter 626 F.S. third degree. By filling out this form, you certify all statements are true and complete to the best of your knowledge and belief. Solstice Benefits, Inc., a licensed Discount Medical Plan Organization under Florida Chapter F.S. 636 Part II and a Licensed Prepaid Limited Health Services Organization under Florida Chapter F.S. 636 Part I and Third Party Administrator under F.S. 626.
SOL3330108 Solstice Benefits, Inc. is a licensed Prepaid Limited Health Services Organization, 7/29/08 Discount Medical Plan Organization under Chapter 636 F.S. and Third Party Administrator under Chapter 626 F.S.